

The American Society of Anesthesiologists score influences on postoperative complications and total hospital charges after laparoscopic colorectal cancer surgery
- PMID: 29718883
- PMCID: PMC6393129
- DOI: 10.1097/MD.0000000000010653
The American Society of Anesthesiologists score influences on postoperative complications and total hospital charges after laparoscopic colorectal cancer surgery
Abstract
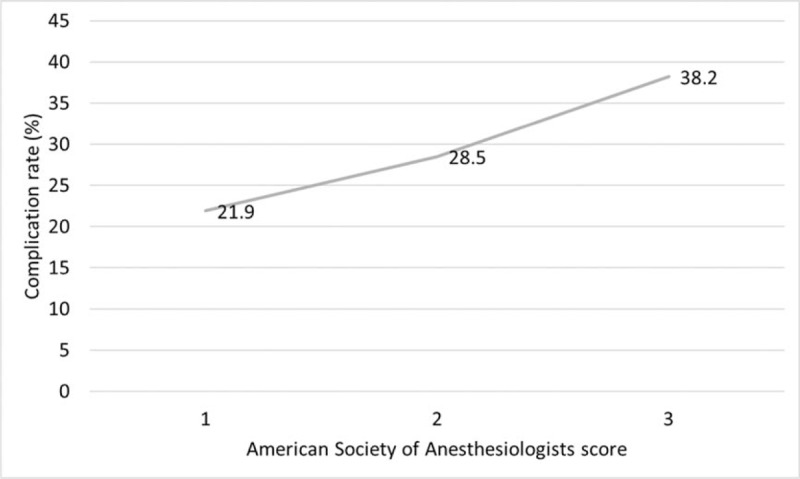
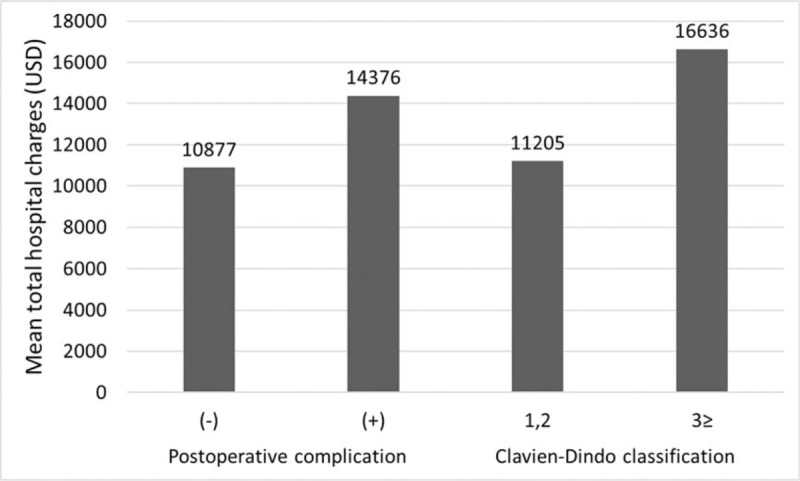
The aim of this study was to investigate the influence of American Society of Anesthesiologists (ASA) scores on postoperative complication rates and total hospital charges following laparoscopic surgery for colorectal cancer.All patients (n = 664) underwent laparoscopic colorectal cancer surgery. A group of patients with an ASA score of 1 or 2 (n = 575) and a group of patients with an ASA score of 3 (n = 89) were compared.The mean age was higher in the group of patients with an ASA score of 3 than in the group of patients with an ASA score of 1 or 2 (70 vs 67 years). The rate of ICU admission (27% vs 15%) was higher in the ASA score 3 group. The mean hospital stay (14 vs 12 days) was longer in the ASA score 3 group. Postoperative 30-day complications (38% vs 27%), 30-day mortality (2% vs 0%), and a Clavien-Dindo classification of ≥3 (21% vs 11%) occurred more frequently in the ASA score 3 group. Mean total hospital charges were significantly higher in the ASA score 3 group (13,906 vs 11,575 USD). Independent risk factors that affected postoperative complications were older age [≥80 years, hazard ratio (HR) = 2.8], an ASA score of 3 (HR = 1.6), and the presence of a primary rectal tumor (HR = 1.6). Postoperative complication rates were 21.9%, 28.5%, and 38.2% in the ASA score 1, 2, and 3 groups, respectively. Total hospital charges were 14,376 USD and 10,877 USD in the groups with and without postoperative complications, respectively. Mean total hospital charges were 10,769 USD, 11,756 USD, and 13,906 USD in the ASA score 1, 2, and 3 groups, respectively.Preoperative ASA scores may be a predictor of postoperative complications and hospital costs when planning laparoscopic surgery for colorectal cancer.
Conflict of interest statement
The authors have no competing interests to declare.
Figures

References
-
- Haynes SR, Lawler PG. An assessment of the consistency of ASA physical status classification allocation. Anaesthesia 1995;50:195–9. - PubMed
-
- Tan WP, Talbott VA, Leong QQ, et al. American Society of Anesthesiologists class and Charlson's comorbidity index as predictors of postoperative colorectal anastomotic leak: a single-institution experience. J Surg Res 2013;184:115–9. - PubMed
-
- Vacanti CJ, VanHouten RJ, Hill RC. A statistical analysis of the relationship of physical status to postoperative mortality in 68,388 cases. Anesth Analg 1970;49:564–6. - PubMed
-
- Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA 2013;309:1599–606. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
