

Increased gut permeability in cancer cachexia: mechanisms and clinical relevance
- PMID: 29719601
- PMCID: PMC5915068
- DOI: 10.18632/oncotarget.24804
Increased gut permeability in cancer cachexia: mechanisms and clinical relevance
Abstract
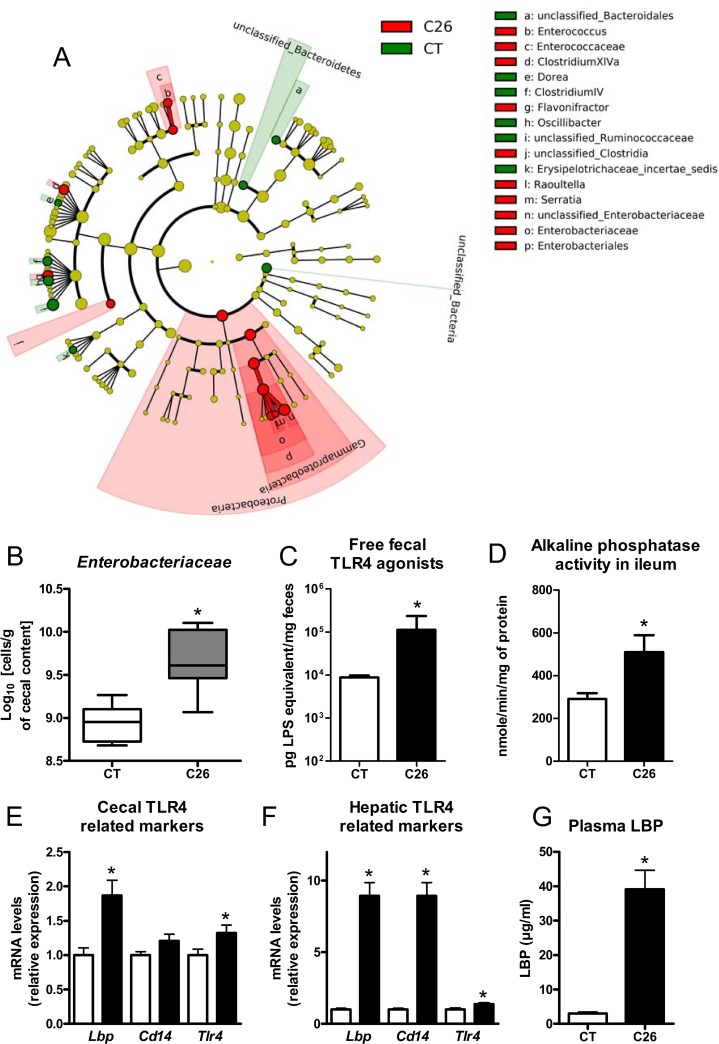
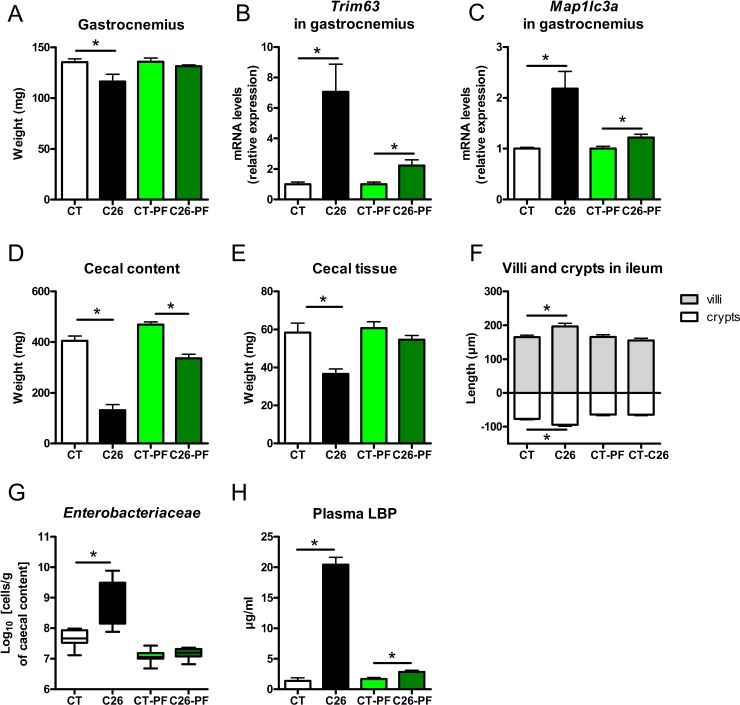
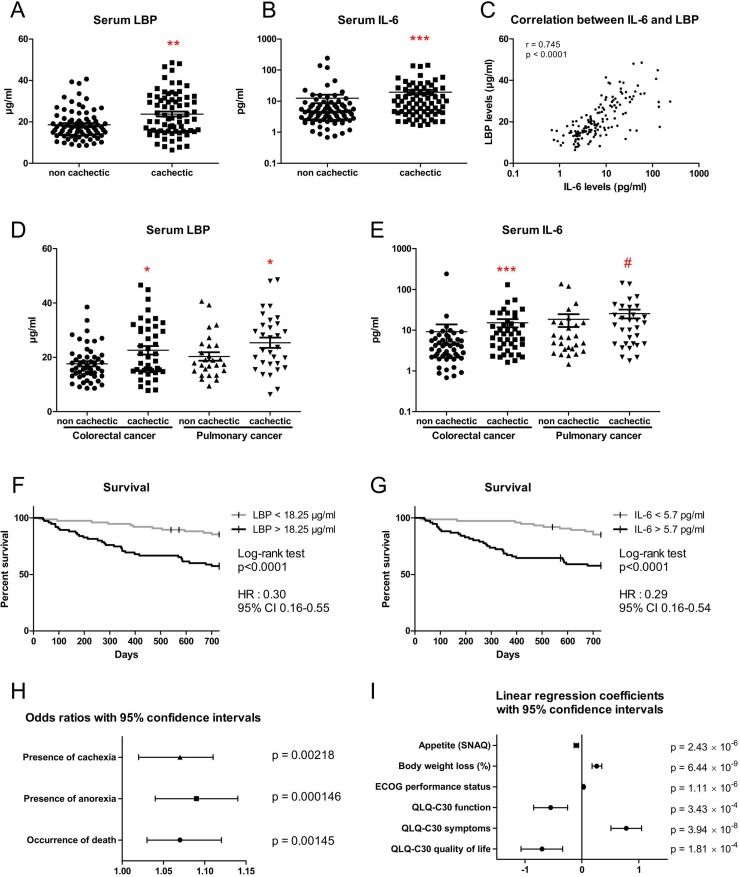
Intestinal disorders often occur in cancer patients, in association with body weight loss, and this alteration is commonly attributed to the chemotherapy. Here, using a mouse model of cancer cachexia induced by ectopic transplantation of C26 cancer cells, we discovered a profound alteration in the gut functions (gut permeability, epithelial turnover, gut immunity, microbial dysbiosis) independently of any chemotherapy. These alterations occurred independently of anorexia and were driven by interleukin 6. Gut dysfunction was found to be resistant to treatments with an anti-inflammatory bacterium (Faecalibacterium prausnitzii) or with gut peptides involved in intestinal cell renewal (teduglutide, a glucagon-like peptide 2 analogue). The translational value of our findings was evaluated in 152 colorectal and lung cancer patients with or without cachexia. The serum level of the lipopolysaccharide-binding protein, often presented as a reflection of the bacterial antigen load, was not only increased in cachectic mice and cancer patients, but also strongly correlated with the serum IL-6 level and predictive of death and cachexia occurrence in these patients. Altogether, our data highlight profound alterations of the intestinal homeostasis in cancer cachexia occurring independently of any chemotherapy and food intake reduction, with potential relevance in humans. In addition, we point out the lipopolysaccharide-binding protein as a new biomarker of cancer cachexia related to gut dysbiosis.
Keywords: Enterobacteriaceae; cancer cachexia; gut barrier function; gut dysbiosis; lipopolysaccharide-binding protein.
Conflict of interest statement
CONFLICTS OF INTEREST The authors declare that they have no competing interests.
Figures



References
-
- Farkas J, von Haehling S, Kalantar-Zadeh K, Morley JE, Anker SD, Lainscak M. Cachexia as a major public health problem: frequent, costly, and deadly. J Cachexia Sarcopenia Muscle. 2013;4:173–78. https://doi.org/10.1007/s13539-013-0105-y. - DOI - PMC - PubMed
-
- von Haehling S, Anker MS, Anker SD. Prevalence and clinical impact of cachexia in chronic illness in Europe, USA, and Japan: facts and numbers update 2016. J Cachexia Sarcopenia Muscle. 2016;7:507–09. https://doi.org/10.1002/jcsm.12167. - DOI - PMC - PubMed
-
- Roy S, Trinchieri G. Microbiota: a key orchestrator of cancer therapy. Nat Rev Cancer. 2017;17:271–85. https://doi.org/10.1038/nrc.2017.13. - DOI - PubMed
-
- Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, Fearon K, Hutterer E, Isenring E, Kaasa S, Krznaric Z, Laird B, Larsson M, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36:11–48. https://doi.org/10.1016/j.clnu.2016.07.015. - DOI - PubMed
-
- Argiles JM, Busquets S, Stemmler B, Lopez-Soriano FJ. Cancer cachexia: understanding the molecular basis. Nat Rev Cancer. 2014;14:754–62. https://doi.org/10.1038/nrc3829. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
