

The effect of implementation strength of basic emergency obstetric and newborn care (BEmONC) on facility deliveries and the met need for BEmONC at the primary health care level in Ethiopia
- PMID: 29720108
- PMCID: PMC5932776
- DOI: 10.1186/s12884-018-1751-z
The effect of implementation strength of basic emergency obstetric and newborn care (BEmONC) on facility deliveries and the met need for BEmONC at the primary health care level in Ethiopia
Abstract
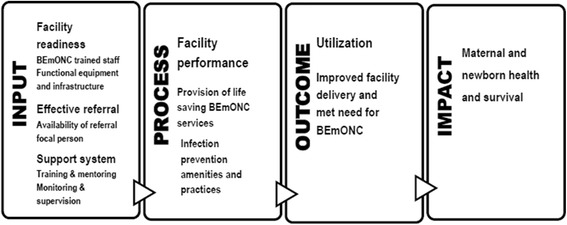
Background: Basic emergency obstetric and newborn care (BEmONC) is a primary health care level initiative promoted in low- and middle-income countries to reduce maternal and newborn mortality. Tailored support, including BEmONC training to providers, mentoring and monitoring through supportive supervision, provision of equipment and supplies, strengthening referral linkages, and improving infection-prevention practice, was provided in a package of interventions to 134 health centers, covering 91 rural districts of Ethiopia to ensure timely BEmONC care. In recent years, there has been a growing interest in measuring program implementation strength to evaluate public health gains. To assess the effectiveness of the BEmONC initiative, this study measures its implementation strength and examines the effect of its variability across intervention health centers on the rate of facility deliveries and the met need for BEmONC.
Methods: Before and after data from 134 intervention health centers were collected in April 2013 and July 2015. A BEmONC implementation strength index was constructed from seven input and five process indicators measured through observation, record review, and provider interview; while facility delivery rate and the met need for expected obstetric complications were measured from service statistics and patient records. We estimated the dose-response relationships between outcome and explanatory variables of interest using regression methods.
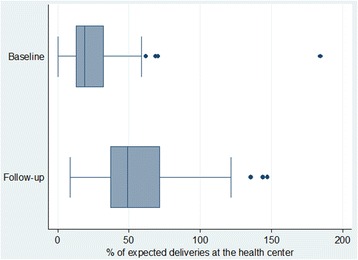
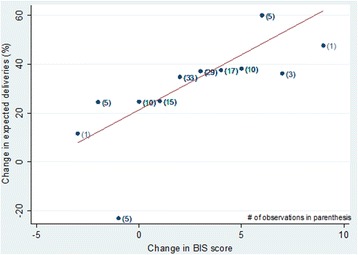
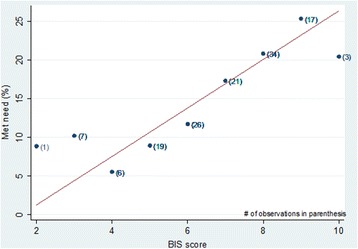
Results: The BEmONC implementation strength index score, which ranged between zero and 10, increased statistically significantly from 4.3 at baseline to 6.7 at follow-up (p < .05). Correspondingly, the health center delivery rate significantly increased from 24% to 56% (p < .05). There was a dose-response relationship between the explanatory and outcome variables. For every unit increase in BEmONC implementation strength score there was a corresponding average of 4.5 percentage points (95% confidence interval: 2.1-6.9) increase in facility-based deliveries; while a higher score for BEmONC implementation strength of a health facility at follow-up was associated with a higher met need.
Conclusion: The BEmONC initiative was effective in improving institutional deliveries and may have also improved the met need for BEmONC services. The BEmONC implementation strength index can be potentially used to monitor the implementation of BEmONC interventions.
Keywords: Basic emergency obstetric and newborn care (BEmONC); Emergency obstetric care (EmONC); Ethiopia; Implementation strength; Life-saving interventions; Low- and middle-income countries (LMIC); Maternal and newborn health; Primary health care; Rural health centers.
Conflict of interest statement
Ethics approval and consent to participate
The ethical review committees of the Amhara, Oromia, SNNP, and Tigray regional health bureaus granted ethical clearance. The study participants (i.e., heads of the health centers and health care providers working in the maternity units) were informed about the purpose of the study and their right to opt-out or not to respond to questions. The study subjects provided informed verbal consent prior to any interview. The interviewer electronically marked the questionnaire as consent given if both the respondents agreed to be interviewed upon listening to the consent statement and then continued with the interview only after receiving and documenting the consent. The survey protocol submitted to the regional health bureaus ethical review committee included the study questionnaire and the consent statement with descriptions of the consent obtaining procedure which was approved by the committee. The name of the respondent was not recorded by the interviewer. Moreover, data collection did not interfere with their normal work with clients. The values, rights, and norms of the study subjects, enumerators and supervisors were respected.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Emergency obstetric care provision in Southern Ethiopia: a facility-based survey.BMJ Open. 2017 Nov 8;7(11):e018459. doi: 10.1136/bmjopen-2017-018459. BMJ Open. 2017. PMID: 29122802 Free PMC article.
-
Current evidence on basic emergency obstetric and newborn care services in Addis Ababa, Ethiopia; a cross sectional study.BMC Pregnancy Childbirth. 2014 Oct 10;14:354. doi: 10.1186/1471-2393-14-354. BMC Pregnancy Childbirth. 2014. PMID: 25300789 Free PMC article.
-
Effects of a participatory community quality improvement strategy on improving household and provider health care behaviors and practices: a propensity score analysis.BMC Pregnancy Childbirth. 2018 Sep 24;18(Suppl 1):364. doi: 10.1186/s12884-018-1977-9. BMC Pregnancy Childbirth. 2018. PMID: 30255783 Free PMC article.
-
Making It Happen: Training health-care providers in emergency obstetric and newborn care.Best Pract Res Clin Obstet Gynaecol. 2015 Nov;29(8):1077-91. doi: 10.1016/j.bpobgyn.2015.03.019. Epub 2015 Apr 4. Best Pract Res Clin Obstet Gynaecol. 2015. PMID: 25911056 Review.
-
Statewide implementation of a quality improvement initiative for reproductive, maternal, newborn and child health and nutritionin Bihar, India.J Glob Health. 2020 Dec;10(2):021008. doi: 10.7189/jogh.10.021008. J Glob Health. 2020. PMID: 33425332 Free PMC article. Review.
Cited by
-
The Effectiveness of Regionalization of Perinatal Care and Specific Facility-Based Interventions: A Systematic Review.Neonatology. 2025;122(Suppl 1):245-261. doi: 10.1159/000541384. Epub 2024 Nov 6. Neonatology. 2025. PMID: 39504943 Free PMC article.
-
Is implementation science a science? Not yet.Front Public Health. 2024 Oct 16;12:1454268. doi: 10.3389/fpubh.2024.1454268. eCollection 2024. Front Public Health. 2024. PMID: 39478746 Free PMC article.
-
The quality of service provision to newborns in the primary healthcare, West Gojjam zone, North-West of Ethiopia: a cross-sectional survey.BMC Pediatr. 2022 Apr 13;22(1):203. doi: 10.1186/s12887-022-03272-8. BMC Pediatr. 2022. PMID: 35418040 Free PMC article.
-
Interventions to improve primary healthcare in rural settings: A scoping review.PLoS One. 2024 Jul 11;19(7):e0305516. doi: 10.1371/journal.pone.0305516. eCollection 2024. PLoS One. 2024. PMID: 38990801 Free PMC article.
-
Repeated measures of implementation variables.Front Health Serv. 2023 Mar 7;3:1085859. doi: 10.3389/frhs.2023.1085859. eCollection 2023. Front Health Serv. 2023. PMID: 36926497 Free PMC article.
References
-
- The Partnership for Maternal Newborn & Child Health . A global review of the key interventions related to Reproductive, Maternal, Newborn and Child Health (RMNCH) Geneva: PMNCH; 2011.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
