

Spectrum of low-density lipoprotein receptor (LDLR) mutations in a cohort of Sri Lankan patients with familial hypercholesterolemia - a preliminary report
- PMID: 29720182
- PMCID: PMC5932885
- DOI: 10.1186/s12944-018-0763-z
Spectrum of low-density lipoprotein receptor (LDLR) mutations in a cohort of Sri Lankan patients with familial hypercholesterolemia - a preliminary report
Abstract
Background: Hypercholesterolemia is a major determinant of cardiovascular disease-associated morbidity and mortality. Mutations in the LDL-receptor (LDLR) gene are implicated in the majority of the cases with familial hypercholesterolemia (FH). However, the spectrum of mutations in the LDLR gene in Sri Lankan patients has not been investigated. The objective of this study was to report the frequency and spectrum of variants in LDLR in a cohort of Sri Lankan patients with FH.
Methods: A series of consecutive patients with FH, diagnosed according to Modified Simon Broome criteria or Dutch Lipid Clinic Network criteria at the University Medical Unit, Colombo, were recruited. Clinical data was recorded. DNA was extracted from peripheral blood samples. The LDLR gene was screened for genetic variants by Sanger sequencing.
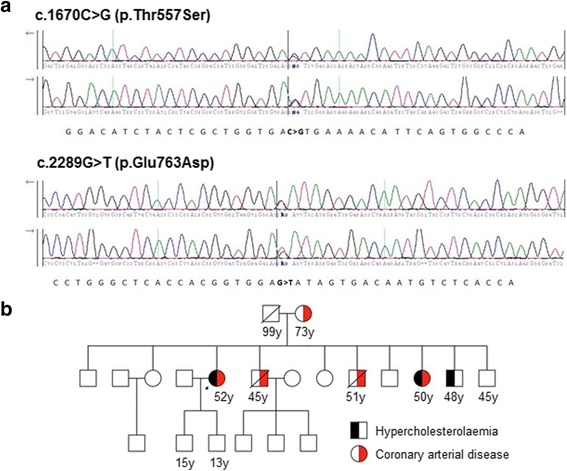
Results: A total of 27 patients [13 (48%) males, 14 (52%) females; age range 24-73 years] were tested. Clinical features found among these 27 patients were: xanthelasma in 5 (18.5%), corneal arcus in 1 (3.7%), coronary artery disease (CAD) in 10 (37%), and a family history of hypercholesterolemia and/or CAD in 24 (88.9%) patients. In the entire cohort, mean total cholesterol was 356.8 mg/dl (±66.4) and mean LDL-cholesterol was 250.3 mg/dl (±67.7). Sanger sequencing of the 27 patients resulted in the identification of known pathogenic missense mutations in 5 (18.5%) patients. Four were heterozygotes for 1 mutation each. They were c.682G > C in 2 patients, c.1720C > A in 1 patient, and c.1855 T > A in 1 patient. One patient with severe FH phenotypes was a compound heterozygote for one known mutation, c.2289G > T, and another missense variant, c.1670C > G (p.Thr557Ser), with unknown functional impact. This latter variant has not been reported in any other population previously.
Conclusions: The frequency of known mutations in the LDLR gene in this cohort of patients was markedly low compared to frequencies reported in other populations. This highlights the likelihood of a complex, polygenic inheritance of FH in Sri Lankan patients, indicating the need for a comprehensive genetic evaluation that includes the screening for mutations in other genes that cause FH, such as APOB, PCSK9, and LDLRAP1.
Keywords: Familial hypercholesterolemia; LDLR gene; Single nucleotide variants (SNV).
Conflict of interest statement
Ethics approval and consent to participate
The study protocol and the form of consent were approved by the Ethics Review Committee, Faculty of Medicine, University of Colombo, Sri Lanka. Written informed consent for the participation in this study and for the genetic testing was obtained from all the participants.
Consent for publication
All the participants provided written informed consent for the publication of the results of this study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Youngblom E, Pariani M, Knowles JW. Familial Hypercholesterolemia. 2014 Jan 2 [Updated 2016 Dec 8]. In: Pagon RA, Adam MP, Ardinger HH, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2017. https://www.ncbi.nlm.nih.gov/books/NBK174884/. Accessed 10 Aug 2017.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
