

Creating a positive perception of childbirth experience: systematic review and meta-analysis of prenatal and intrapartum interventions
- PMID: 29720201
- PMCID: PMC5932889
- DOI: 10.1186/s12978-018-0511-x
Creating a positive perception of childbirth experience: systematic review and meta-analysis of prenatal and intrapartum interventions
Abstract
Background: A negative experience in childbirth is associated with chronic maternal morbidities. The aim of this systematic review and meta-analysis was to identify currently available successful interventions to create a positive perception of childbirth experience which can prevent psychological birth trauma.
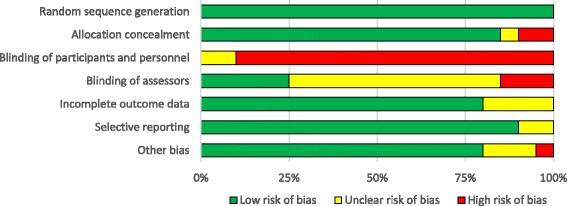
Methods: Randomized controlled trials of interventions in pregnancy or labour which aimed to improve childbirth experience versus usual care were identified from 1994 to September 2016. Low risk pregnant or childbearing women were chosen as the study population. PEDRO scale and Cochrane risk of bias tool were used for quality assessment. Pooled effect estimates were calculated when more than two studies had similar intervention. If it was not possible to include a study in the meta-analysis, its data were summarized narratively.
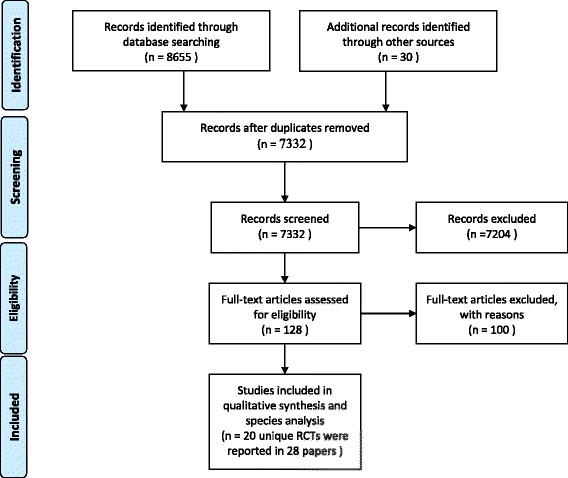
Results: After screening of 7832 titles/abstracts, 20 trials including 22,800 participants from 12 countries were included. Successful strategies to create a positive perception of childbirth experience were supporting women during birth (Risk Ratio = 1.35, 95% Confidence Interval: 1.07 to 1.71), intrapartum care with minimal intervention (Risk Ratio = 1.29, 95% Confidence Interval:1.15 to 1.45) and birth preparedness and readiness for complications (Mean Difference = 3.27, 95% Confidence Interval: 0.66 to 5.88). Most of the relaxation and pain relief strategies were not successful to create a positive birth experience (Mean Difference = - 2.64, 95% Confidence Intervention: - 6.80 to 1.52).
Conclusion: The most effective strategies to create a positive birth experience are supporting women during birth, intrapartum care with minimal intervention and birth preparedness. This study might be helpful in clinical approaches and designing future studies about prevention of the negative and traumatic birth experiences.
Keywords: Childbirth experience; Psychological birth trauma; Support; Systematic review.
Conflict of interest statement
Ethics approval and consent to participate
This research was ethically approved by Tehran University of Medical sciences ethics committee (reference No IR.TUMS.VCR.REC.1395.374).
Competing interests
The authors declare that have no competing interest that may be relevant to the submitted work.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
