

Greater rate of cephalic screw mobilisation following proximal femoral nailing in hip fractures with a tip-apex distance (TAD) and a calcar referenced TAD greater than 25 mm
- PMID: 29720223
- PMCID: PMC5930512
- DOI: 10.1186/s13018-018-0814-1
Greater rate of cephalic screw mobilisation following proximal femoral nailing in hip fractures with a tip-apex distance (TAD) and a calcar referenced TAD greater than 25 mm
Abstract
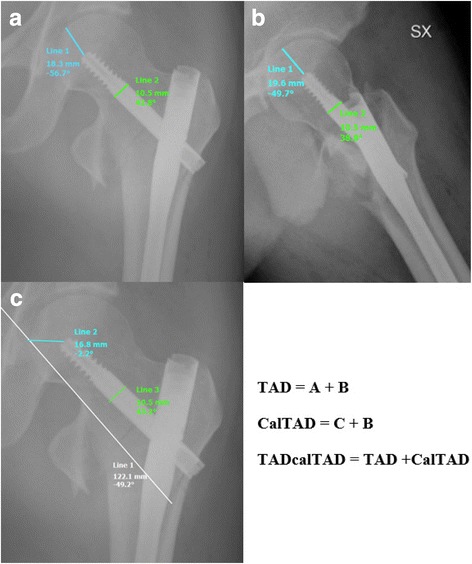
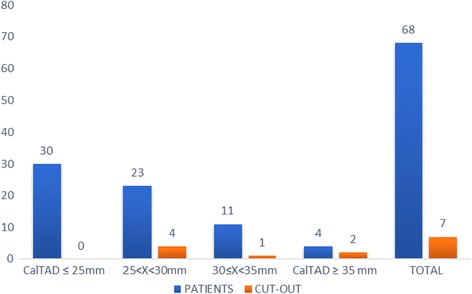
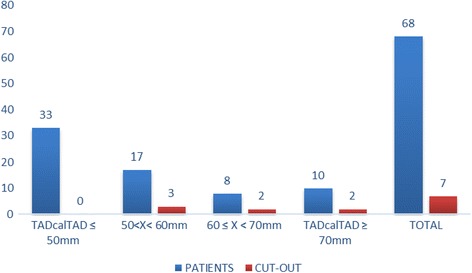
Background: To ascertain whether the tip-apex distance (TAD), calcar referenced TAD (CalTAD), and the sum of both (TADcalTAD) are predictive measurements of mobilisation of the cephalic screw in patients with trochanteric hip fractures.
Methods: Between 2014 and 2015, 68 patients (mean age 86 years, 45 females, 23 males) with a trochanteric hip fracture underwent intramedullary nailing. The TAD and CalTAD were measured, and for each parameter, we calculated sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
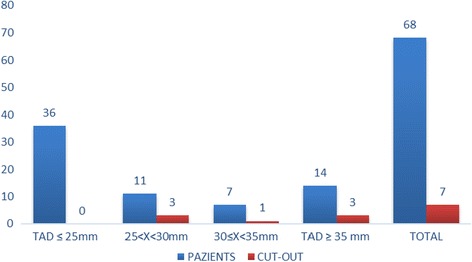
Results: There is evidence of a statistically significant association between a TAD and CalTAD greater than 25 mm and a TADcalTAD greater than 50 mm and mobilisation of the cephalic screw. All measurements have similar sensitivity, but the TAD presents the highest specificity (p < 0.01).
Conclusion: To avoid the risk of mobilisation of the cephalic screw and possible subsequent failure of the construct, surgeons should strive for a TAD and CalTAD less than 25 mm and a TADcalTAD less than 50 mm when using intramedullary fixation.
Keywords: CalTAD; Fracture; Hip; TAD; TADcalTAD.
Conflict of interest statement
Ethics approval and consent to participate
All patients provided signed informed consent. In accordance with Italian law, ethics committee approval was not obtained, as the study was purely retrospective, with no changes to standard clinical practice. According to Italian law, when patients sign an informed consent for an operation, they automatically consent to be included in studies detailing the outcomes of their treatment.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Rose S, Maffulli N. Hip fractures. An epidemiological review. Bull Hosp Jt Dis. 1999;58:197–201. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
