

Two versus five days of antibiotics after appendectomy for complex acute appendicitis (APPIC): study protocol for a randomized controlled trial
- PMID: 29720238
- PMCID: PMC5932884
- DOI: 10.1186/s13063-018-2629-0
Two versus five days of antibiotics after appendectomy for complex acute appendicitis (APPIC): study protocol for a randomized controlled trial
Abstract
Background: Acute appendicitis is one of the most common indications for emergency surgery. In patients with a complex appendicitis, prolonged antibiotic prophylaxis is recommended after appendectomy. There is no consensus regarding the optimum duration of antibiotics. Guidelines propose 3 to 7 days of treatment, but shorter courses may be as effective in the prevention of infectious complications. At the same time, the global issue of increasing antimicrobial resistance urges for optimization of antibiotic strategies. The aim of this study is to determine whether a short course (48 h) of postoperative antibiotics is non-inferior to current standard practice of 5 days.
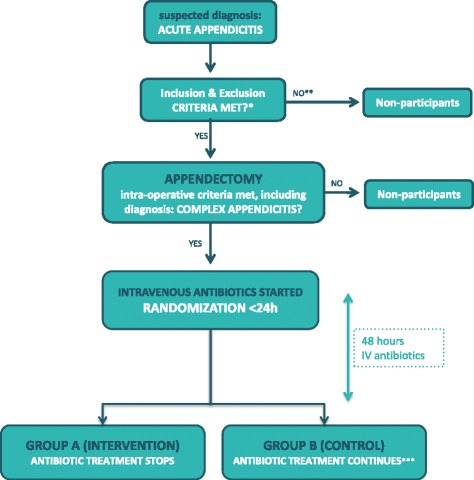
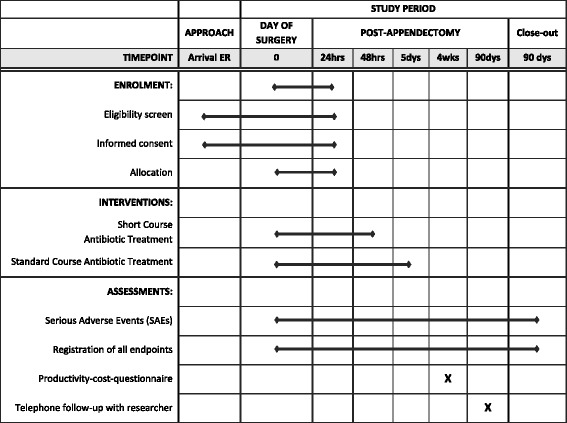
Methods: Patients of 8 years and older undergoing appendectomy for acute complex appendicitis - defined as a gangrenous and/or perforated appendicitis or appendicitis in presence of an abscess - are eligible for inclusion. Immunocompromised or pregnant patients are excluded, as well as patients with a contraindication to the study antibiotics. In total, 1066 patients will be randomly allocated in a 1:1 ratio to the experimental treatment arm (48 h of postoperative intravenously administered (IV) antibiotics) or the control arm (5 days of postoperative IV antibiotics). After discharge from the hospital, patients participate in a productivity-cost-questionnaire at 4 weeks and a standardized telephone follow-up at 90 days after appendectomy. The primary outcome is a composite endpoint of infectious complications, including intra-abdominal abscess (IAA) and surgical site infection (SSI), and mortality within 90 days after appendectomy. Secondary outcomes include IAA, SSI, restart of antibiotics, length of hospital stay (LOS), reoperation, percutaneous drainage, readmission rate, and cost-effectiveness. The non-inferiority margin for the difference in the primary endpoint rate is set at 7.5% (one-sided test at ɑ 0.025). Both per-protocol and intention-to-treat analyses will be performed.
Discussion: This trial will provide evidence on whether 48 h of postoperative antibiotics is non-inferior to a standard course of 5 days of antibiotics. If non-inferiority is established, longer intravenous administration following appendectomy for complex appendicitis can be abandoned, and guidelines need to be adjusted accordingly.
Trial registration: Dutch Trial Register, NTR6128 . Registered on 20 December 2016.
Keywords: .; Acute appendicitis; Antibiotic prophylaxis; Complex appendicitis.
Conflict of interest statement
Ethics approval and consent to participate
This study will be carried out in accordance with the principles of the Declaration of Helsinki and in compliance with Good Clinical Practice. The study protocol was approved on March 14 2017 by the Ethics Committee of the Erasmus MC Rotterdam in the Netherlands (MEC2016–719). Secondary approval from local boards is obtained before initiation in each participating center. Any substantial amendments to the original study dossier will be submitted for approval to the Ethics Committee in line with regulatory requirements. So far, five substantial amendments have been submitted and approved. In the first amendment generalized peritonitis was discarded as an exclusion criterion (in the original protocol) and the definition of adverse events was narrowed to events related to the experimental treatment. In the second amendment, ceftriaxone-metronidazole was incorporated in the protocol as an alternative to cefuroxime-metronidazole and gentamicin was approved as co-intervention. Moreover, in all five amendments participating centers were added, to add up to 14 participating centers in total.
Eligible patients will receive detailed information regarding the trial, both orally and in writing (Additional file 2). Written informed consent will be obtained from all participants by surgeons and surgical residents from the participating centers. All participants are protected by the liability insurance of the Erasmus MC that is in accordance with the legal requirements in the Netherlands. Data will be handled confidentially and anonymously. Upon inclusion into this study, each patient will be assigned a study number. The key to the code, a subject identification code list, will be stored separately safeguarded by the local investigator. The code will not be based on the patient’s initials or birth date. Only involved investigators will have access to the data. The handling of personal data is in compliance with the Dutch Personal Data Protection Act (in Dutch: De Wet Bescherming Persoonsgegevens, Wbp). The results of the present study will be disseminated through publication in a general medical or surgical journal and presentation at international conferences.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Vons C, Barry C, Maitre S, Pautrat K, Leconte M, Costaglioli B, et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Lancet. 2011;377(9777):1573–1579. doi: 10.1016/S0140-6736(11)60410-8. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
