

High Rate of Infection by Only Oncogenic Human Papillomavirus in Amerindians
- PMID: 29720524
- PMCID: PMC5932372
- DOI: 10.1128/mSphere.00176-18
High Rate of Infection by Only Oncogenic Human Papillomavirus in Amerindians
Abstract
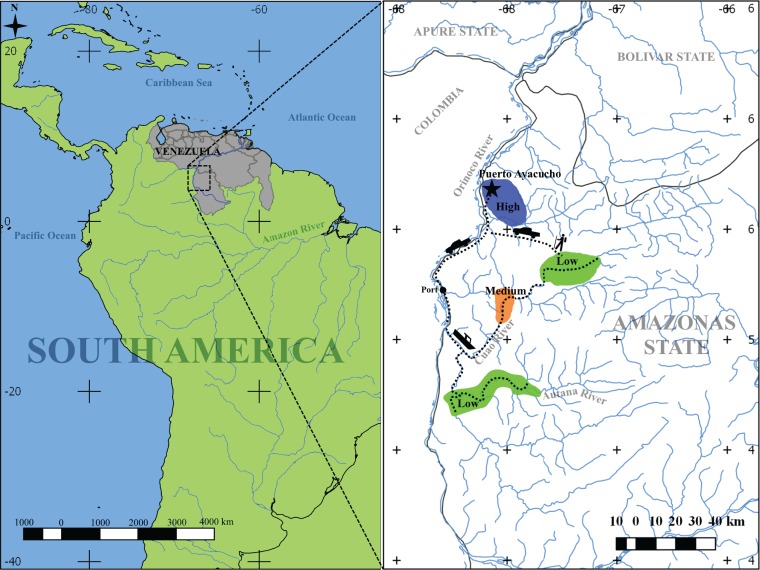
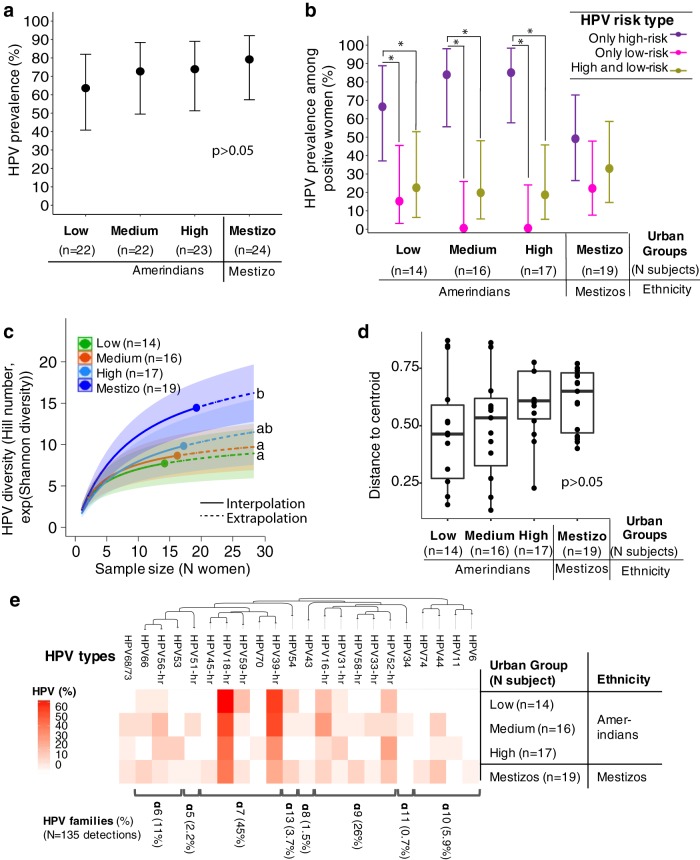
Human papillomavirus (HPV), an etiological agent of cervical cancer (CC), has infected humans since ancient times. Amerindians are the furthest migrants out of Africa, and they reached the Americas more than 14,000 years ago. Some groups still remain isolated, and some migrate to towns, forming a gradient spanning urbanization. We hypothesized that, by virtue of their history, lifestyle, and isolation from the global society, remote Amerindian women have lower HPV diversity than do urban women (Amerindian or mestizo). Here we determined the diversity of the 25 most relevant cervical HPV types in 82 Amerindians spanning urbanization (low, medium, and high, consistent with the exposure to urban lifestyles of the town of Puerto Ayacucho in the Venezuelan Amazonas State), and in 29 urban mestizos from the town. Cervical, anal, oral, and introitus samples were taken, and HPVs were typed using reverse DNA hybridization. A total of 23 HPV types were detected, including 11 oncogenic or high-risk types, most associated with CC. Cervical HPV prevalence was 75%, with no differences by group, but Amerindians from low and medium urbanization level had significantly lower HPV diversity than mestizos did. In Amerindians, but not in mestizos, infections by only high-risk HPVs were higher than coinfections or by exclusively low-risk HPVs. Cervical abnormalities only were observed in Amerindians (9/82), consistent with their high HPV infection. The lower cervical HPV diversity in more isolated Amerindians is consistent with their lower exposure to the global pool, and transculturation to urban lifestyles could have implications on HPV ecology, infection, and virulence.IMPORTANCE The role of HPV type distribution on the disparity of cervical cancer (CC) incidence between human populations remains unknown. The incidence of CC in the Amazonas State of Venezuela is higher than the national average. In this study, we determined the diversity of known HPV types (the viral agent of CC) in Amerindian and mestizo women living in the Venezuelan Amazonas State. Understanding the ecological diversity of HPV in populations undergoing lifestyle transformations has important implication on public health measures for CC prevention.
Keywords: diversity; human papillomavirus; lifestyle; oncogenic virus; urbanization.
Copyright © 2018 Vargas-Robles et al.
Figures
References
-
- zur Hausen H, Gissmann L, Steiner W, Dippold W, Dreger I. 1975. Human papilloma viruses and cancer. Bibl Haematol 1975:569–571. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
