

Cluster Headache: Epidemiology, Pathophysiology, Clinical Features, and Diagnosis
- PMID: 29720812
- PMCID: PMC5909131
- DOI: 10.4103/aian.AIAN_349_17
Cluster Headache: Epidemiology, Pathophysiology, Clinical Features, and Diagnosis
Abstract
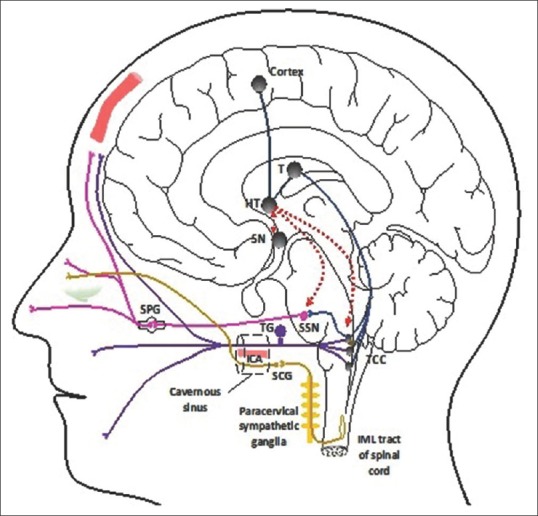
Cluster headache is a primary headache disorder affecting up to 0.1% of the population. Patients suffer from cluster headache attacks lasting from 15 to 180 min up to 8 times a day. The attacks are characterized by the severe unilateral pain mainly in the first division of the trigeminal nerve, with associated prominent unilateral cranial autonomic symptoms and a sense of agitation and restlessness during the attacks. The male-to-female ratio is approximately 2.5:1. Experimental, clinical, and neuroimaging studies have advanced our understanding of the pathogenesis of cluster headache. The pathophysiology involves activation of the trigeminovascular complex and the trigeminal-autonomic reflex and accounts for the unilateral severe headache, the prominent ipsilateral cranial autonomic symptoms. In addition, the circadian and circannual rhythmicity unique to this condition is postulated to involve the hypothalamus and suprachiasmatic nucleus. Although the clinical features are distinct, it may be misdiagnosed, with patients often presenting to the otolaryngologist or dentist with symptoms. The prognosis of cluster headache remains difficult to predict. Patients with episodic cluster headache can shift to chronic cluster headache and vice versa. Longitudinally, cluster headache tends to remit with age with less frequent bouts and more prolonged periods of remission in between bouts.
Keywords: Cluster headache; diagnosis; epidemiology; pathophysiology; trigeminal autonomic cephalalgias.
Conflict of interest statement
Peter James Goadsby reports grants and personal fees from Allergan, Amgen, and Eli-Lilly and Company; personal fees from Akita Biomedical, Alder Biopharmaceuticals, Avanir Pharma, Cipla Ltd., Dr Reddy's Laboratories, eNeura, Electrocore LLC, Novartis, Pfizer Inc., Quest Diagnostics Scion, Teva Pharmaceuticals, Trigemina Inc., Scion; personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Massachusetts Medical Society, Oxford University Press; and in addition, Dr. Goadsby has a patent Magnetic stimulation for headache assigned, without fee, to eNeura.
Figures
References
-
- Koehler PJ. Prevalence of headache in Tulp's Observationes Medicae (1641) with a description of cluster headache. Cephalalgia. 1993;13:318–20. - PubMed
-
- Harris W. Neuritis and Neuralgia. 1st ed. London: Humphrey Milford, Oxford University Press; 1926.
-
- Boes CJ, Capobianco DJ, Matharu MS, Goadsby PJ. Wilfred Harris’ early description of cluster headache. Cephalalgia. 2002;22:320–6. - PubMed
-
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38:1–211. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
