

The diversity of myeloid immune cells shaping wound repair and fibrosis in the lung
- PMID: 29721324
- PMCID: PMC5911451
- DOI: 10.1002/reg2.97
The diversity of myeloid immune cells shaping wound repair and fibrosis in the lung
Abstract
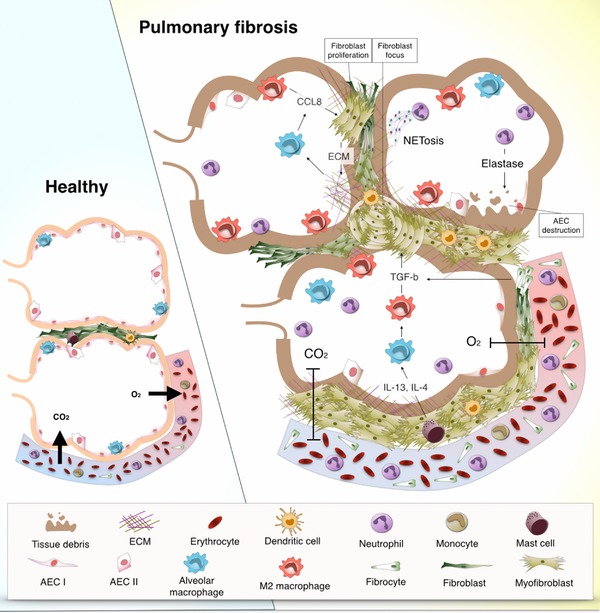
In healthy circumstances the immune system coordinates tissue repair responses in a tight balance that entails efficient inflammation for removal of potential threats, proper wound closure, and regeneration to regain tissue function. Pathological conditions, continuous exposure to noxious agents, and even ageing can dysregulate immune responses after injury. This dysregulation can lead to a chronic repair mechanism known as fibrosis. Alterations in wound healing can occur in many organs, but our focus lies with the lung as it requires highly regulated immune and repair responses with its continuous exposure to airborne threats. Dysregulated repair responses can lead to pulmonary fibrosis but the exact reason for its development is often not known. Here, we review the diversity of innate immune cells of myeloid origin that are involved in tissue repair and we illustrate how these cell types can contribute to the development of pulmonary fibrosis. Moreover, we briefly discuss the effect of age on innate immune responses and therefore on wound healing and we conclude with the implications of current knowledge on the avenues for future research.
Keywords: dendritic cells; fibrocytes; macrophages; monocytes; neutrophils.
Figures

References
-
- Aldenborg, F. , Nilsson, K. , Jarlshammar, B. , Bjermer, L. , & Enerback, L. (1993). Mast cells and biogenic amines in radiation‐induced pulmonary fibrosis. American Journal of Respiratory Cell and Molecular Biology, 8(1), 112–117. - PubMed
-
- Andersson, C. K. , Mori, M. , Bjermer, L. , Lofdahl, C. G. , & Erjefalt, J. S. (2010). Alterations in lung mast cell populations in patients with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine, 181(3), 206–217. - PubMed
-
- Andersson‐Sjöland, A. , Garc, C. , Nihlberg, K. , Becerril, C. , Ram, R. , Pardo, A. , … Selman, M. (2008). Fibrocytes are a potential source of lung fibroblasts in idiopathic pulmonary fibrosis. International Journal of Biochemistry and Cell Biology, 40(10), 2129–2140. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources