

Surgical approach to the intrathoracic goiter
- PMID: 29721546
- PMCID: PMC5915827
- DOI: 10.1002/lio2.146
Surgical approach to the intrathoracic goiter
Abstract
Objective: In a retrospective study, the authors analyzed the surgical approach to the intrathoracic goiter to avoid sternotomy or thoracotomy.
Methods: We selected 70 intrathoracic cases of multinodular goiter out of 988 cases of thyroidectomy and compared them with cervical goiter cases. Surgical technique, results, and postsurgical complications were assessed.
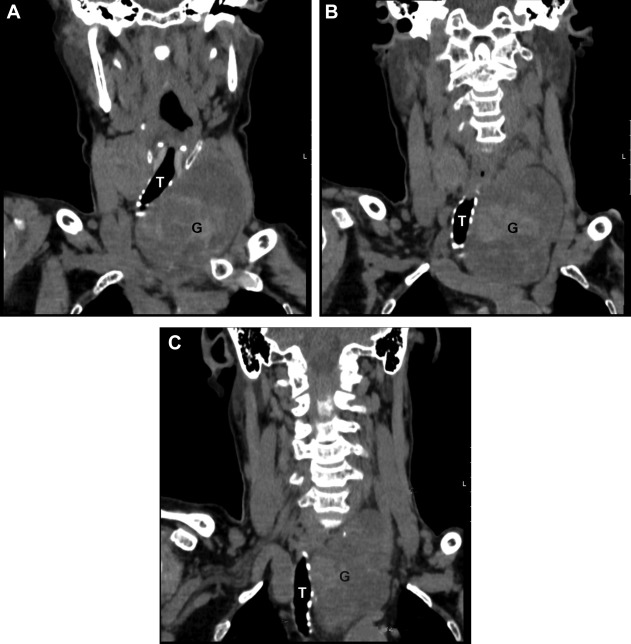
Results: The analyzed cases presented the retrosternal goiter (n = 53; 75.7%), the retrotracheal goiter (n = 9; 12.8%), and the retroesophageal goiter (n = 8; 11.4%). Complaining of chest pressure or discomfort was specific for intrathoracic cases (50%; 35 of 70). All goiters except one were removed via cervical incision. The surgeons used head reclination and isthmus dissection when removing sizable goiters. Mean weight of goiters was 180 g. The recurrent laryngeal nerve was more often temporarily damaged in intrathoracic cases in comparison with cervical cases (4.3% vs. 2.8%, P = .04), but the difference in permanent injury was less significant (P = .09). The incidence of temporary hypoparathyroidism was significantly higher in intrathoracic cases (P = .01).
Conclusion: In cases of multinodular goiter the goiters of various extensions can be successfully removed via the cervical incision in most of the cases even if they occupy the retrosternal, retrotracheal, or retroesophageal position. The transthoracic approaches and sternotomy might be justified in malignant cases.
Level of evidence: 4.
Keywords: Intrathoracic goiter; retrosternal goiter; surgery; thoracotomy.
Figures


References
-
- Lilienthal H. A case of mediastinal thyroid removed by transsternal mediastinotomy. Surg Gynecol Obstet 1915;20:589.
-
- Hertzler AE. Diseases of the Thyroid Gland. St. Louis: Mosby Company; 1922, p. 148.
-
- Vadasz P, Kotsis L. Surgical aspects of 175 mediastinal goiters. Eur J Cardiothorac Surg 1998;14:393–397. - PubMed
-
- Wright CD, Mathisen DJ. Mediastinal tumors: diagnosis and treatment. World J Surg 2001;25:204–209. - PubMed
-
- Netterville JL, Coleman SC, Smith JC, Smith MM, Day TA, Burkey BB. Management of substernal goiter. Laryngoscope 1998;108:1611–1617. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials