

Review
doi: 10.3390/jcm7050101.
Gastrodoudenal Embolization: Indications, Technical Pearls, and Outcomes
Affiliations
- PMID: 29724061
- PMCID: PMC5977140
- DOI: 10.3390/jcm7050101
Item in Clipboard
Review
Gastrodoudenal Embolization: Indications, Technical Pearls, and Outcomes
J Clin Med.
.
Abstract
The gastroduodenal artery (GDA) is frequently embolized in cases of upper GI bleed that has failed endoscopic therapy. Additionally, it may be done for GDA pseudoaneurysms or as an adjunctive procedure prior to Yttrim-90 (Y90) treatment of hepatic tumors. This clinical review will summarize anatomy and embryology of the GDA, indications, outcomes and complications of GDA embolization.
Keywords: gastroduodenal artery; pseudoaneurysm; upper GI bleed embolization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
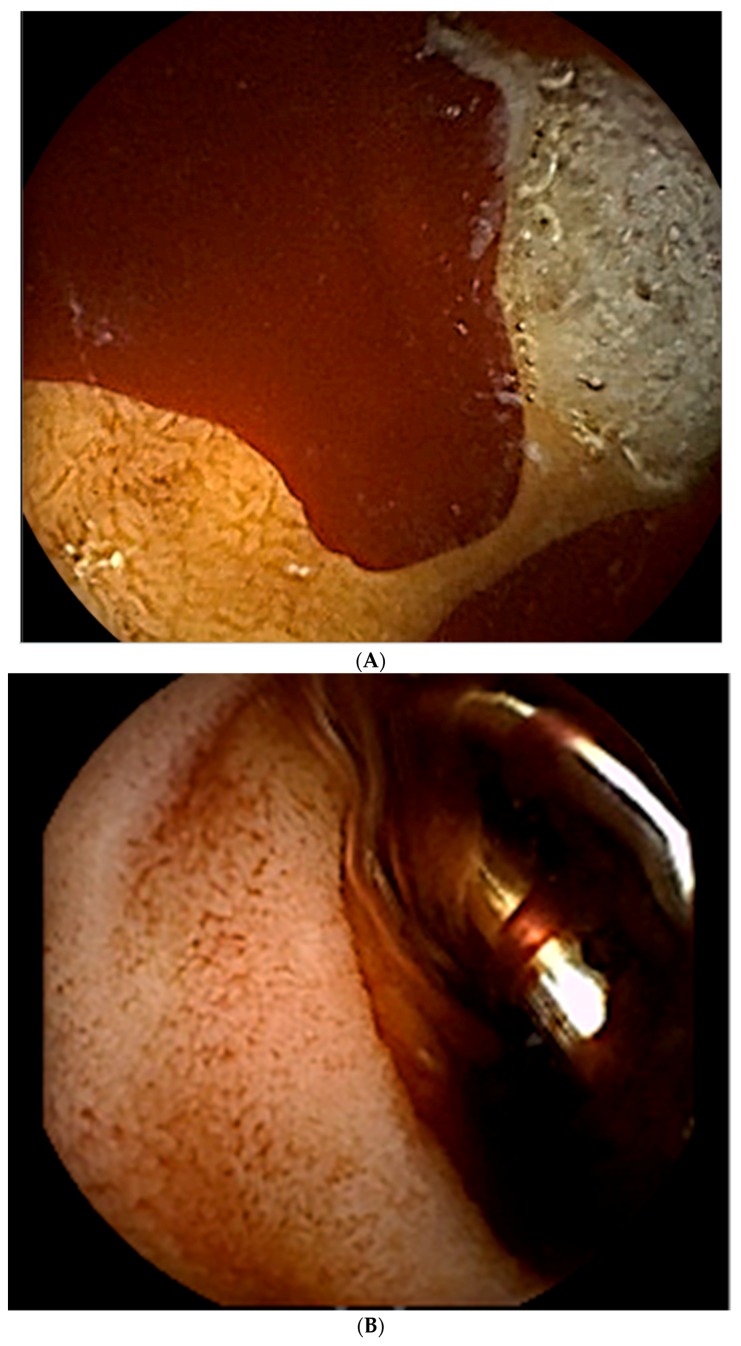
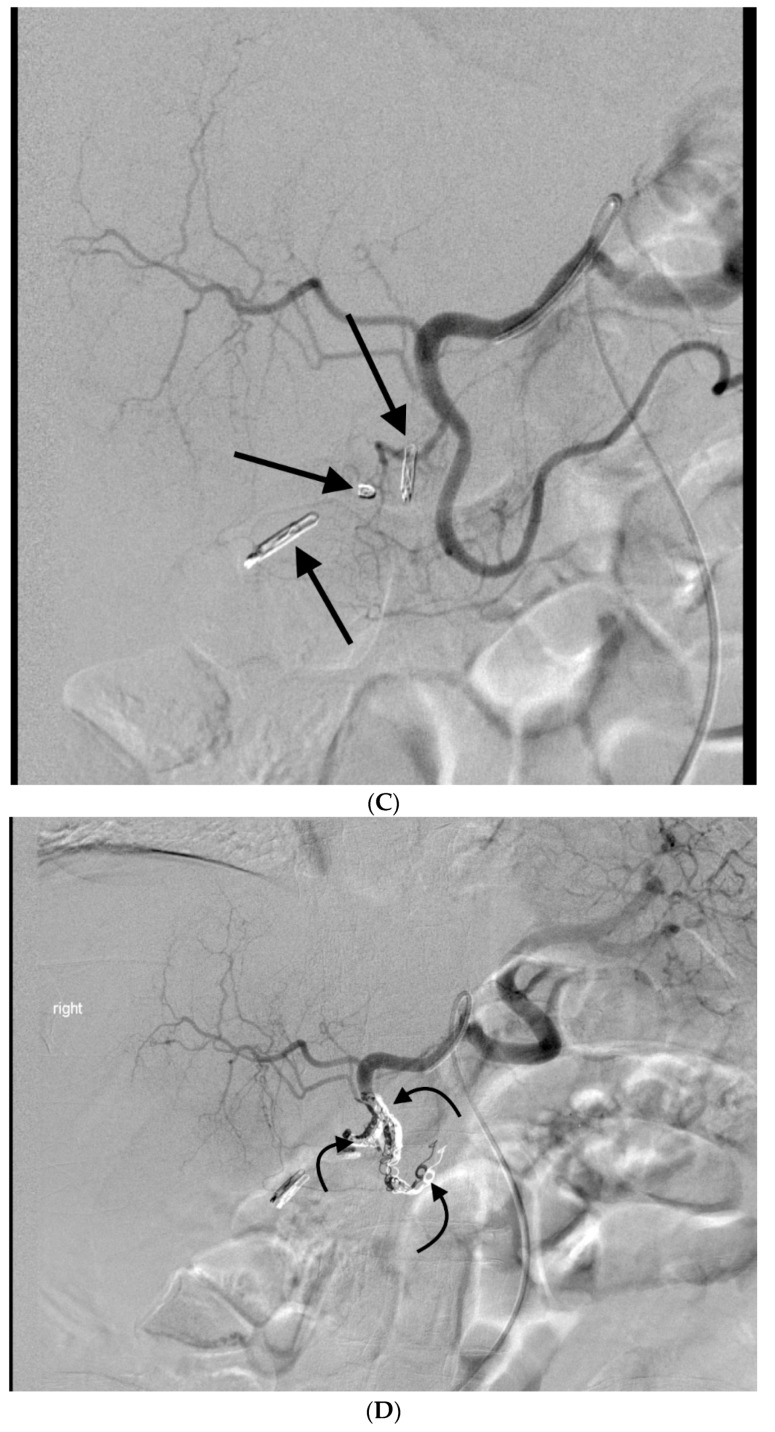
This 72 year old man presented with hematemesis and melena. (A) He underwent an upper endoscopy, at which time blood was seen in the duodenal bulb with two cratered oozing ulcers present. The largest ulcer was 10 mm in diameter. (B) The ulcers were treated with an injection of 4cc of 1:10,000 epinephrine, followed by the placement of hemostatic clips. (C) While hemostasis was achieved at the time of endoscopy, the patient rebled 3 h later. An angiogram shows multiple endoscopic clips (black arrows) in the duodenum, a region supplied by the gastrodoudenal artery (GDA). These clips helped to guide the angiographer to the location of the bleed. The (D) coil (curved black arrows) and gelfoam embolization was performed on the GDA.
This 72 year old man presented with hematemesis and melena. (A) He underwent an upper endoscopy, at which time blood was seen in the duodenal bulb with two cratered oozing ulcers present. The largest ulcer was 10 mm in diameter. (B) The ulcers were treated with an injection of 4cc of 1:10,000 epinephrine, followed by the placement of hemostatic clips. (C) While hemostasis was achieved at the time of endoscopy, the patient rebled 3 h later. An angiogram shows multiple endoscopic clips (black arrows) in the duodenum, a region supplied by the gastrodoudenal artery (GDA). These clips helped to guide the angiographer to the location of the bleed. The (D) coil (curved black arrows) and gelfoam embolization was performed on the GDA.
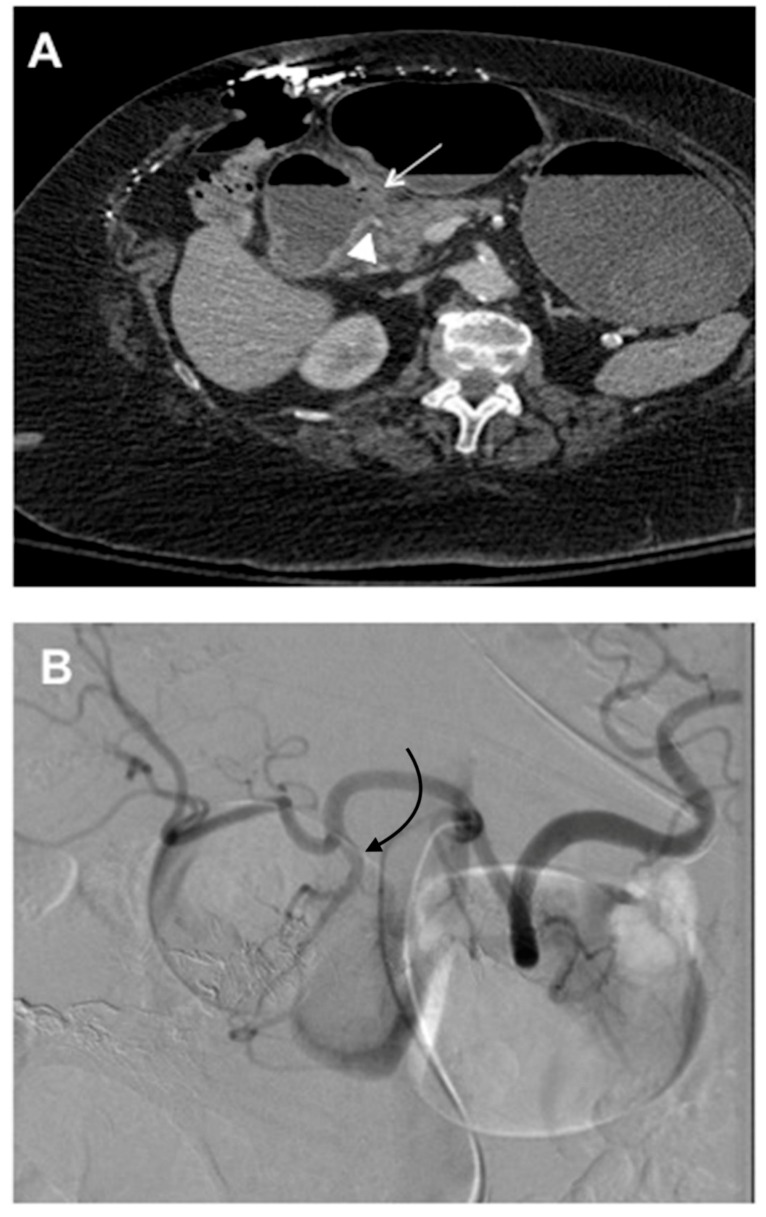
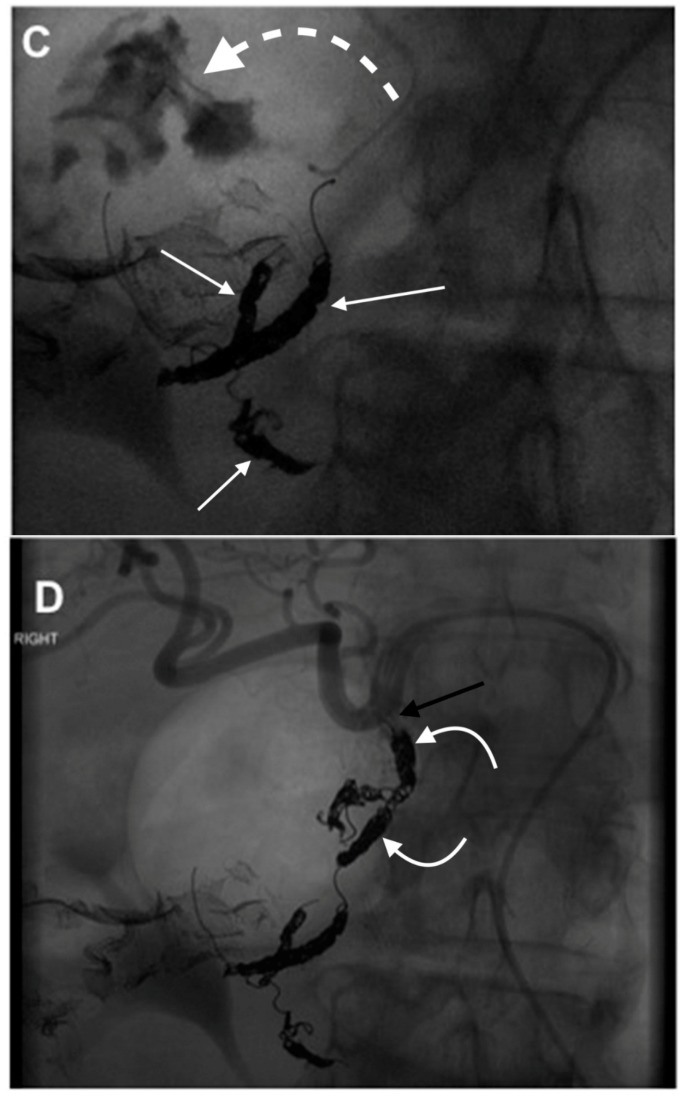
This 78 year old woman presented with melena, hematemesis, hypotension, and acute blood loss anemia. An endoscopy was not performed, given the high volume of blood which was felt to likely obscure the (A) Computerized Tomography (CT) images, demonstrating the duodenal perforation (white arrow) in the posterior wall with abnormal appearing GDA coursing directly adjacent to the perforation (white arrowhead). The (B) celiac angiogram shows the origin of the GDA (curved black arrow). The (C) branches of the GDA that were distal to the duodenal ulcer were coil emobolized (white straight arrows) and the repeat angiogram from the proximal to mid GDA, showed a contrast extravasation into the duodenum (curved dashed arrow). (D) Coil embolization (curved white arrows) was done across and proximal to the site of the extravasation up to the origin of the GDA from the common hepatic artery (black arrow).
This 78 year old woman presented with melena, hematemesis, hypotension, and acute blood loss anemia. An endoscopy was not performed, given the high volume of blood which was felt to likely obscure the (A) Computerized Tomography (CT) images, demonstrating the duodenal perforation (white arrow) in the posterior wall with abnormal appearing GDA coursing directly adjacent to the perforation (white arrowhead). The (B) celiac angiogram shows the origin of the GDA (curved black arrow). The (C) branches of the GDA that were distal to the duodenal ulcer were coil emobolized (white straight arrows) and the repeat angiogram from the proximal to mid GDA, showed a contrast extravasation into the duodenum (curved dashed arrow). (D) Coil embolization (curved white arrows) was done across and proximal to the site of the extravasation up to the origin of the GDA from the common hepatic artery (black arrow).
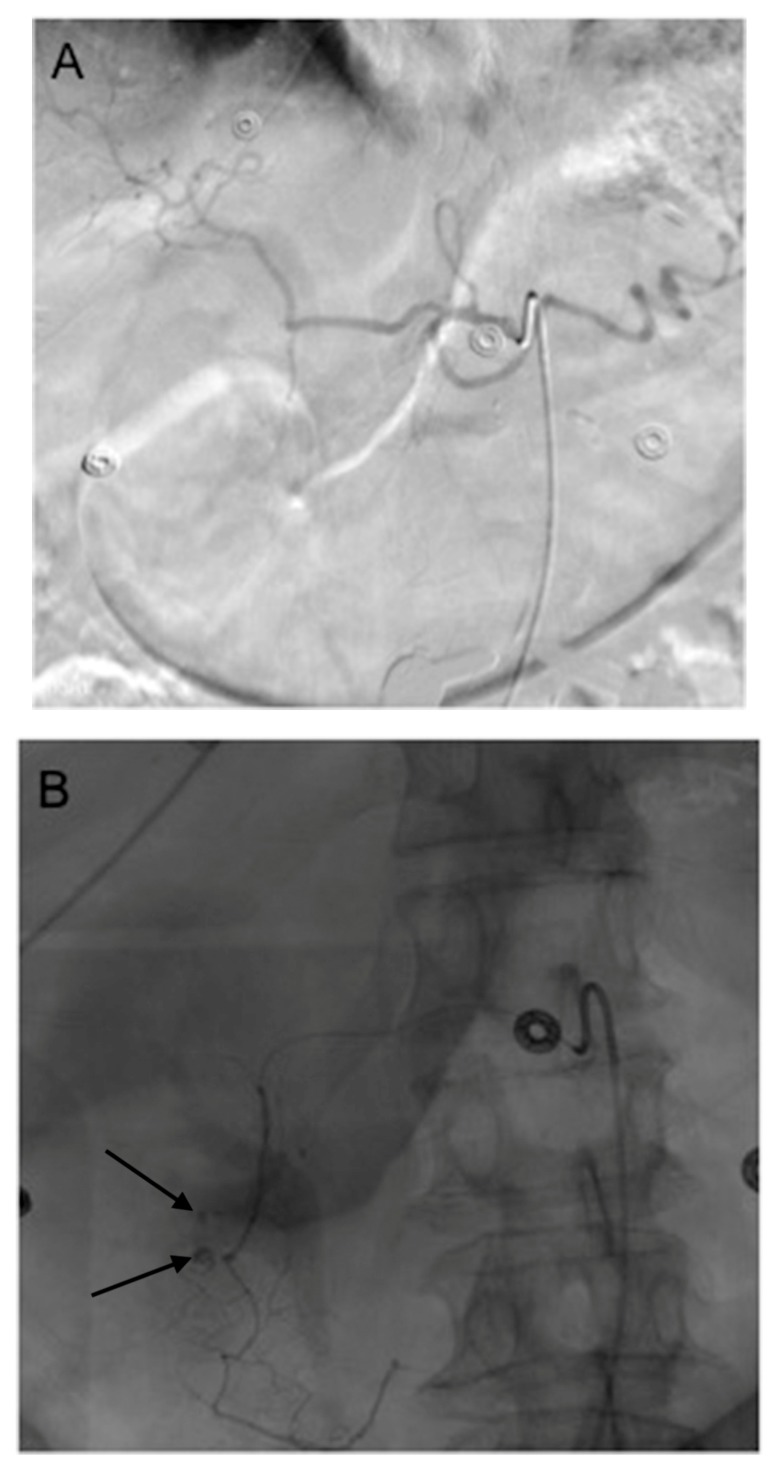
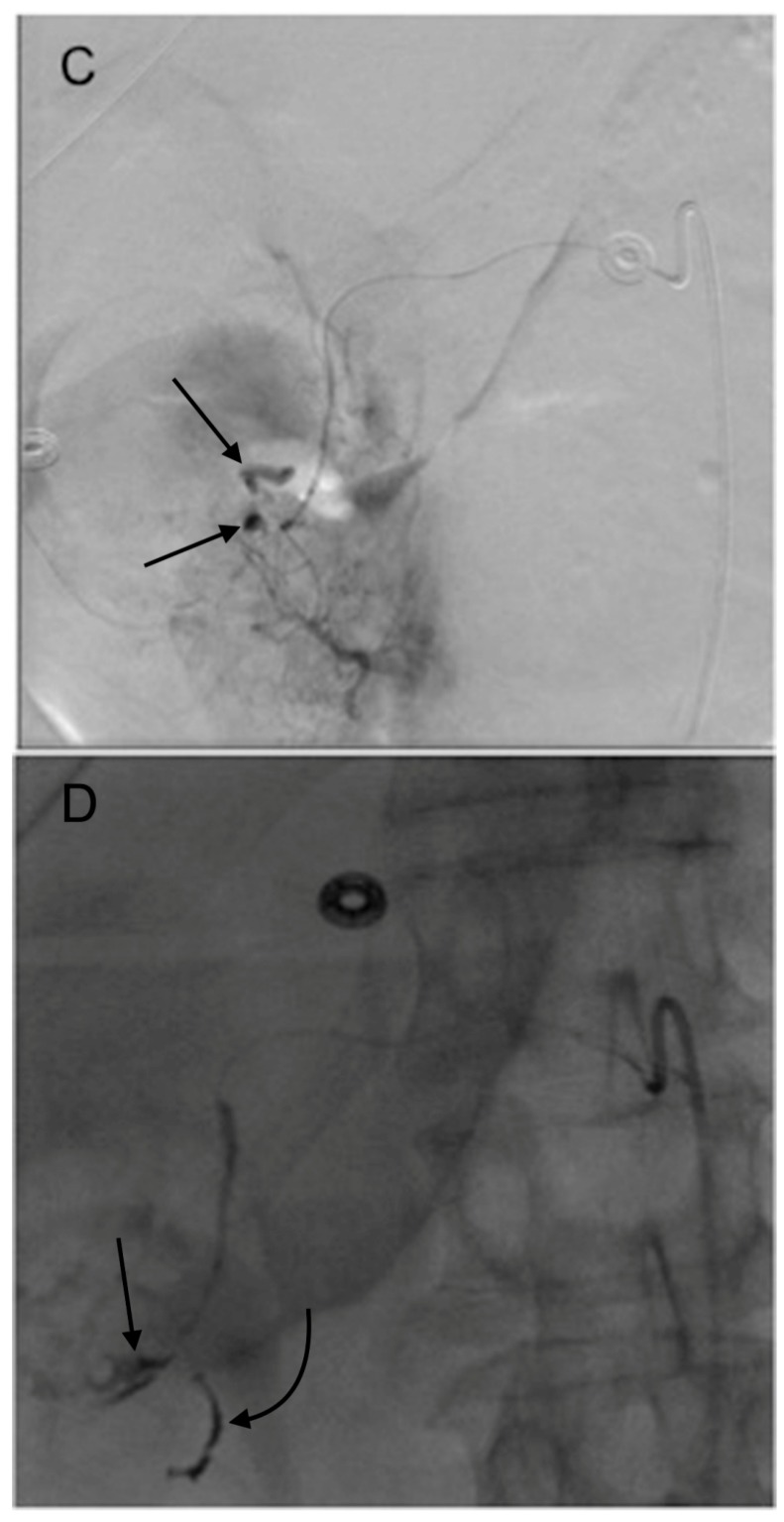
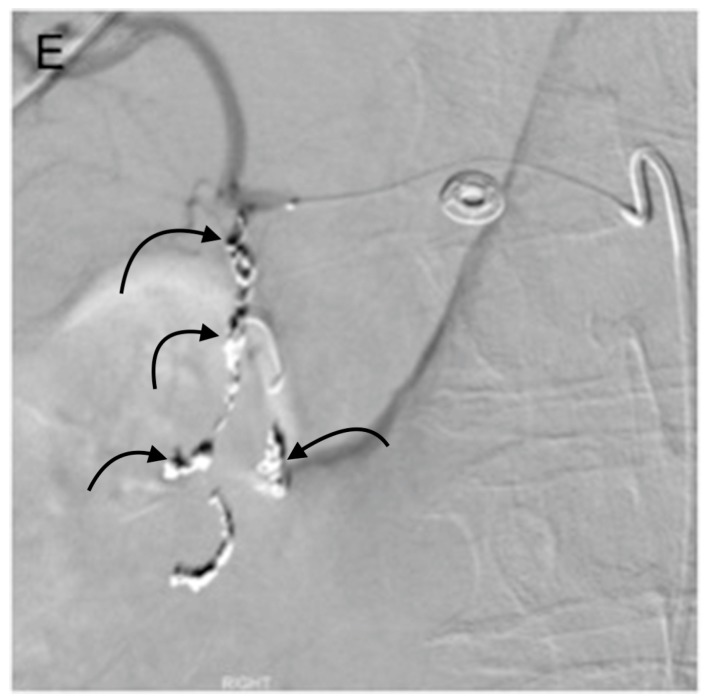
This 77 year old woman had a known history of multiple gastric and duodenal ulcers, and presented with massive upper gastrointestinal (GI) bleeding. A (A) celiac angiogram showed severely clamped down vessels that were consistent with hypotensive state and vasopressor use. The (B) native and (C) subtracted images show multiple sites of extravasation (black arrows). The coils embolization (black curved arrow) was done distal to the extravasation (black straight arrow) (D) and back to the origin of the GDA as it arose from the common hepatic artery (E). The bleeding was successful stopped.
This 77 year old woman had a known history of multiple gastric and duodenal ulcers, and presented with massive upper gastrointestinal (GI) bleeding. A (A) celiac angiogram showed severely clamped down vessels that were consistent with hypotensive state and vasopressor use. The (B) native and (C) subtracted images show multiple sites of extravasation (black arrows). The coils embolization (black curved arrow) was done distal to the extravasation (black straight arrow) (D) and back to the origin of the GDA as it arose from the common hepatic artery (E). The bleeding was successful stopped.
This 77 year old woman had a known history of multiple gastric and duodenal ulcers, and presented with massive upper gastrointestinal (GI) bleeding. A (A) celiac angiogram showed severely clamped down vessels that were consistent with hypotensive state and vasopressor use. The (B) native and (C) subtracted images show multiple sites of extravasation (black arrows). The coils embolization (black curved arrow) was done distal to the extravasation (black straight arrow) (D) and back to the origin of the GDA as it arose from the common hepatic artery (E). The bleeding was successful stopped.

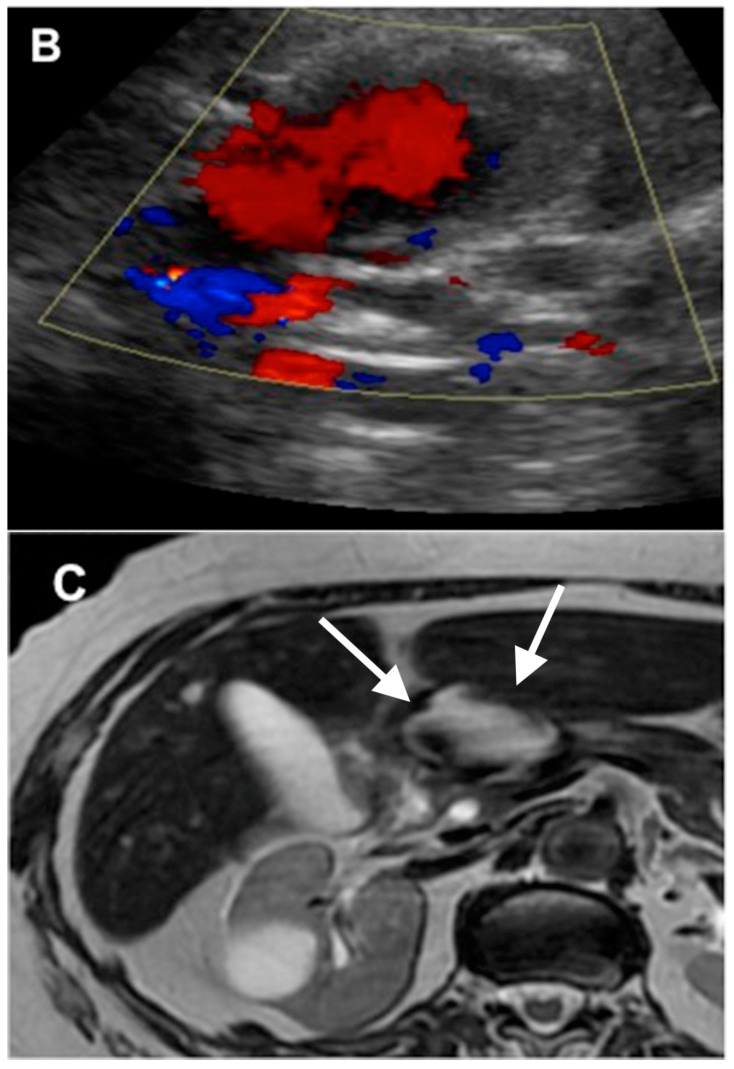
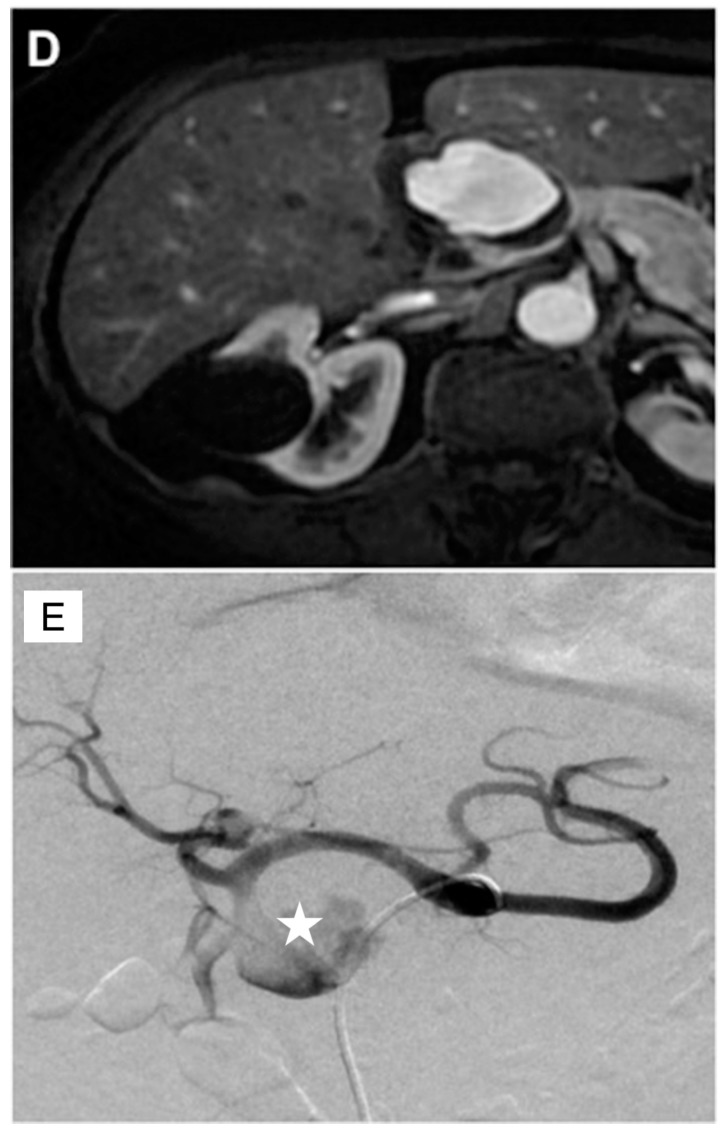
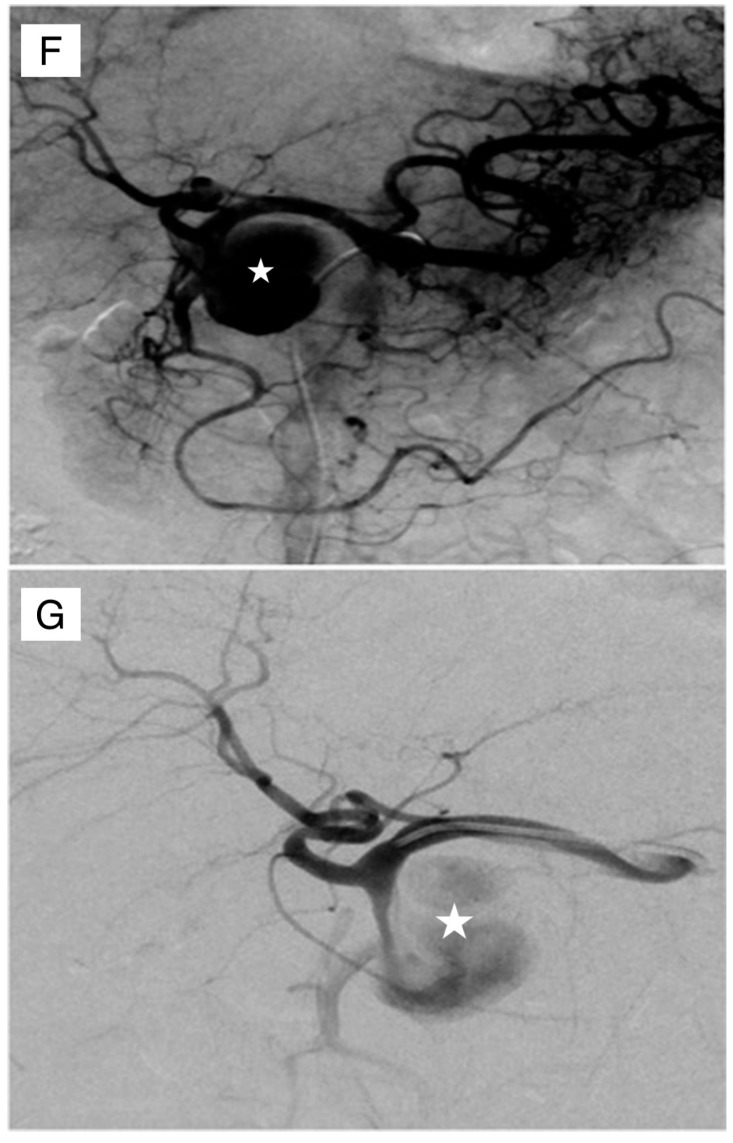
This 75 year old female with chronic pancreatitis secondary to pancreatic divisum who presented with worsening abdominal pain and early satiety. The (A) transverse abdominal ultrasound showing hypoechoic cystic structure (white star), separate from the gallbladder. The (B) color Doppler showed this to be highly vascular (aneurysm or pseudoaneurysm). The (C) T2 weighted abdominal magnetic resonance imaging (MRI) showed the mixed signal intensity within this aneurysm (white arrows). The (D) contrast enhanced imaging in the arterial phase showed the filling of this pseudoaneurysm with some peripheral thrombus. The patient was brought to angiography for an urgent angiogram and embolization. The celiac angiogram in the (E) early arterial and (F) parenchymal phase showed the large pseudoaneurysm (white star) arising from the GDA. The (G) common hepatic artery angiogram showed similar findings. The (H) embolization was then done. The coils were first placed distal to the pseudoaneurysm (curved black arrow), then within the pseudoaneurysm (straight black arrows), and then within the GDA that was proximal to the pseudoaneurysm (dashed black arrow). The (I) superior mesenteric (SMA) injection showed no backdoor filling of the pseudoaneursym. Again, the coils were seen distal to the sac (curved black arrow), as well as within the sac (straight black arrows).
This 75 year old female with chronic pancreatitis secondary to pancreatic divisum who presented with worsening abdominal pain and early satiety. The (A) transverse abdominal ultrasound showing hypoechoic cystic structure (white star), separate from the gallbladder. The (B) color Doppler showed this to be highly vascular (aneurysm or pseudoaneurysm). The (C) T2 weighted abdominal magnetic resonance imaging (MRI) showed the mixed signal intensity within this aneurysm (white arrows). The (D) contrast enhanced imaging in the arterial phase showed the filling of this pseudoaneurysm with some peripheral thrombus. The patient was brought to angiography for an urgent angiogram and embolization. The celiac angiogram in the (E) early arterial and (F) parenchymal phase showed the large pseudoaneurysm (white star) arising from the GDA. The (G) common hepatic artery angiogram showed similar findings. The (H) embolization was then done. The coils were first placed distal to the pseudoaneurysm (curved black arrow), then within the pseudoaneurysm (straight black arrows), and then within the GDA that was proximal to the pseudoaneurysm (dashed black arrow). The (I) superior mesenteric (SMA) injection showed no backdoor filling of the pseudoaneursym. Again, the coils were seen distal to the sac (curved black arrow), as well as within the sac (straight black arrows).
This 75 year old female with chronic pancreatitis secondary to pancreatic divisum who presented with worsening abdominal pain and early satiety. The (A) transverse abdominal ultrasound showing hypoechoic cystic structure (white star), separate from the gallbladder. The (B) color Doppler showed this to be highly vascular (aneurysm or pseudoaneurysm). The (C) T2 weighted abdominal magnetic resonance imaging (MRI) showed the mixed signal intensity within this aneurysm (white arrows). The (D) contrast enhanced imaging in the arterial phase showed the filling of this pseudoaneurysm with some peripheral thrombus. The patient was brought to angiography for an urgent angiogram and embolization. The celiac angiogram in the (E) early arterial and (F) parenchymal phase showed the large pseudoaneurysm (white star) arising from the GDA. The (G) common hepatic artery angiogram showed similar findings. The (H) embolization was then done. The coils were first placed distal to the pseudoaneurysm (curved black arrow), then within the pseudoaneurysm (straight black arrows), and then within the GDA that was proximal to the pseudoaneurysm (dashed black arrow). The (I) superior mesenteric (SMA) injection showed no backdoor filling of the pseudoaneursym. Again, the coils were seen distal to the sac (curved black arrow), as well as within the sac (straight black arrows).
This 75 year old female with chronic pancreatitis secondary to pancreatic divisum who presented with worsening abdominal pain and early satiety. The (A) transverse abdominal ultrasound showing hypoechoic cystic structure (white star), separate from the gallbladder. The (B) color Doppler showed this to be highly vascular (aneurysm or pseudoaneurysm). The (C) T2 weighted abdominal magnetic resonance imaging (MRI) showed the mixed signal intensity within this aneurysm (white arrows). The (D) contrast enhanced imaging in the arterial phase showed the filling of this pseudoaneurysm with some peripheral thrombus. The patient was brought to angiography for an urgent angiogram and embolization. The celiac angiogram in the (E) early arterial and (F) parenchymal phase showed the large pseudoaneurysm (white star) arising from the GDA. The (G) common hepatic artery angiogram showed similar findings. The (H) embolization was then done. The coils were first placed distal to the pseudoaneurysm (curved black arrow), then within the pseudoaneurysm (straight black arrows), and then within the GDA that was proximal to the pseudoaneurysm (dashed black arrow). The (I) superior mesenteric (SMA) injection showed no backdoor filling of the pseudoaneursym. Again, the coils were seen distal to the sac (curved black arrow), as well as within the sac (straight black arrows).
This 75 year old female with chronic pancreatitis secondary to pancreatic divisum who presented with worsening abdominal pain and early satiety. The (A) transverse abdominal ultrasound showing hypoechoic cystic structure (white star), separate from the gallbladder. The (B) color Doppler showed this to be highly vascular (aneurysm or pseudoaneurysm). The (C) T2 weighted abdominal magnetic resonance imaging (MRI) showed the mixed signal intensity within this aneurysm (white arrows). The (D) contrast enhanced imaging in the arterial phase showed the filling of this pseudoaneurysm with some peripheral thrombus. The patient was brought to angiography for an urgent angiogram and embolization. The celiac angiogram in the (E) early arterial and (F) parenchymal phase showed the large pseudoaneurysm (white star) arising from the GDA. The (G) common hepatic artery angiogram showed similar findings. The (H) embolization was then done. The coils were first placed distal to the pseudoaneurysm (curved black arrow), then within the pseudoaneurysm (straight black arrows), and then within the GDA that was proximal to the pseudoaneurysm (dashed black arrow). The (I) superior mesenteric (SMA) injection showed no backdoor filling of the pseudoaneursym. Again, the coils were seen distal to the sac (curved black arrow), as well as within the sac (straight black arrows).
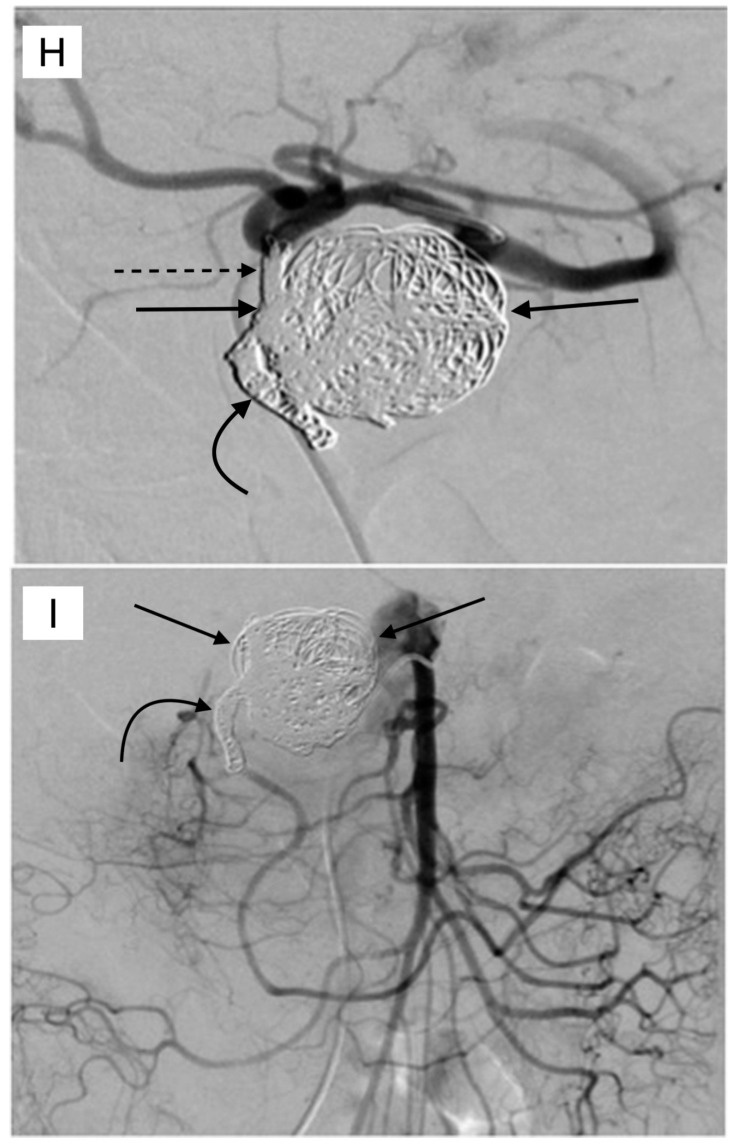
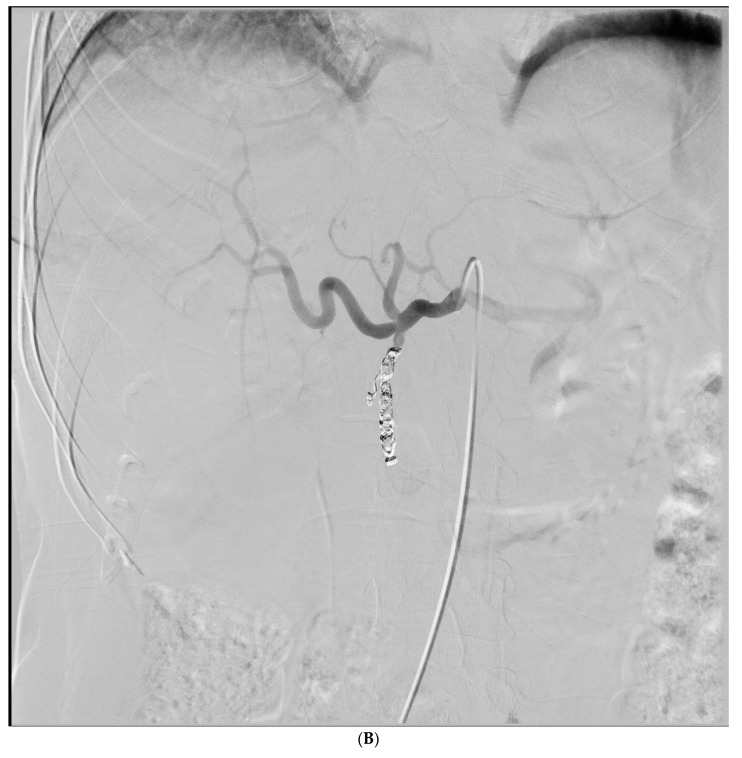
This 48 year old female with metastatic colo-rectal cancer was referred for selective internal radiation therapy, using Yittrium-90. The (A) mapping angiogram showed a trifurcation of the common hepatic artery into the GDA (dashed arrow), left hepatic (curved arrow), and right hepatic (straight arrow) arteries. GDA embolization with this anatomic configuration was felt to be necessary in order to reduce the chances of the non-target duodenal embolization. The (B) GDA was successfully cannulated with a microcatheter, and multiple coils were placed successfully, which embolized this vessel. The Yttrium-90 (Y-90) administration was subsequently performed without clinical or radiographic evidence of non-target embolization to the duodenum.
This 48 year old female with metastatic colo-rectal cancer was referred for selective internal radiation therapy, using Yittrium-90. The (A) mapping angiogram showed a trifurcation of the common hepatic artery into the GDA (dashed arrow), left hepatic (curved arrow), and right hepatic (straight arrow) arteries. GDA embolization with this anatomic configuration was felt to be necessary in order to reduce the chances of the non-target duodenal embolization. The (B) GDA was successfully cannulated with a microcatheter, and multiple coils were placed successfully, which embolized this vessel. The Yttrium-90 (Y-90) administration was subsequently performed without clinical or radiographic evidence of non-target embolization to the duodenum.
References
-
- Som P., Grapin-Botton A. The Current Embryology of the Foregut and Its Derivatives. Neurographics. 2016;6:43–63. doi: 10.3174/ng.1160142. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
