

Microbial keratitis-induced endophthalmitis: incidence, symptoms, therapy, visual prognosis and outcomes
- PMID: 29724209
- PMCID: PMC5934862
- DOI: 10.1186/s12886-018-0777-3
Microbial keratitis-induced endophthalmitis: incidence, symptoms, therapy, visual prognosis and outcomes
Abstract
Background: To evaluate symptoms, therapies and outcomes in rare microbial keratitis-induced endophthalmitis.
Methods: Retrospective study with 11 patients treated between 2009 and 2014. Clinical findings, corneal diseases, history of steroids and trauma, use of contact lenses, number and type of surgical interventions, determination of causative organisms and visual acuity (VA) were evaluated.
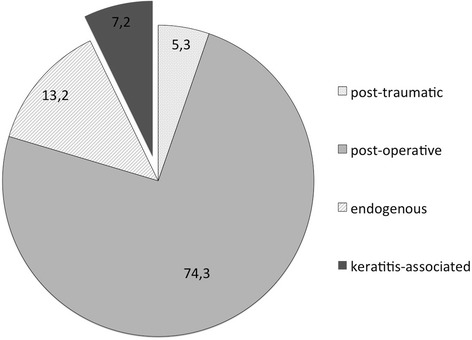
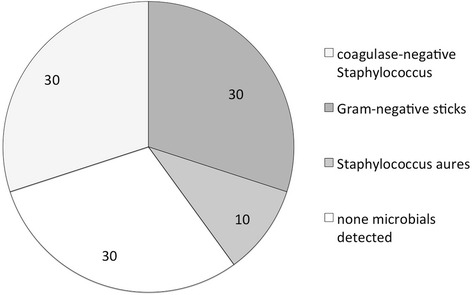
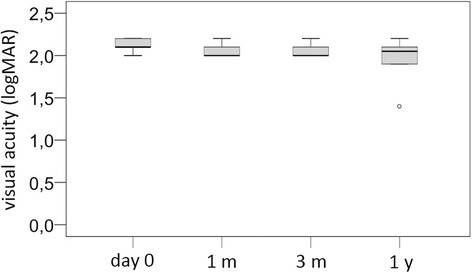
Results: The incidence of transformation from microbial keratitis to an endophthalmitis was 0.29% (n = 11/3773). In 90.9% (n = 10/11), there were pre-existent eyelid and corneal problems, in 45.5% (n = 5/11) rubeosis iridis with increased intraocular pressure and corneal decompensation, and in 18.2% (n = 2/11), ocular trauma. Specimens could be obtained in 10 of 11 samples: 33.3% of those 10 specimens were Gram-positive coagulase-negative Staphylococci (n = 3/10) or Gram-negative rods (n = 3/10) and 10.0% Staphylococcus aureus (n = 1/10). In 30% (n = 3/10), no pathogens were identifiable. 72.7% (n = 8/11) of all keratitis-induced endophthalmitis were treated with vitrectomy and 9.1% (n = 1/11) with amniotic-membrane transplantation. In 27.3% (n = 3/11) the infected eye had to be enucleated - 18.2% (n = 2/11) primarily, 9.1% (n = 1/11) secondarily. No patient suffered from sympathetic ophthalmia. The median initial VA was 2.1 logMAR (n = 11/11). At one month, median VA was 2.0 logMAR (n = 7/11), after three months 2.0 logMAR (n = 6/11), and after one year 2.05 logMAR (n = 6/11). The change in VA was not significant (p > 0.99). 36.4% (n = 4/11) of the cases resulted in blindness.
Conclusions: The overall outcome is poor. Enucleation should be weighed against the risk of local and systemic spread of the infection, prolonged rehabilitation and sympathetic ophthalmia.
Keywords: Corneal ulcer; Endophthalmitis; Enucleation; Infection; Keratitis.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the internal Institutional Review Board of Klinikum rechts der Isar, Technical University of Munich.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
