

Financial management of large, multi-center trials in a challenging funding milieu
- PMID: 29724229
- PMCID: PMC5934907
- DOI: 10.1186/s13063-018-2638-z
Financial management of large, multi-center trials in a challenging funding milieu
Abstract
Background: Randomized clinical trials that have public health implications but no or low potential for commercial gain are predominantly funded by governmental (e.g., National Institutes of Health (NIH)) and not-for-profit organizations. Our objective was to develop an alternative clinical trial site funding model for judicious allocation of declining public research funds.
Methods: In the Vitamin D and Type 2 Diabetes (D2d) study, an NIH-supported, large clinical trial testing the effect of vitamin D supplementation on incident diabetes in 2423 participants at high risk for diabetes, a hybrid financial management model for supporting collaborating clinical sites was developed and applied. The funding model employed two reimbursement components: Core (for study start-up and partial efforts throughout the study, ~40% of the total site budget), invoiced by sites, and Performance-Based Payments (for successful enrollment of participants and completion of follow-up visits, ~60% of the total site budget), automatically issued to the sites by the Coordinating Center based on actual recruitment and visits conducted. Underperforming sites transitioned to Performance-Based Payments only.
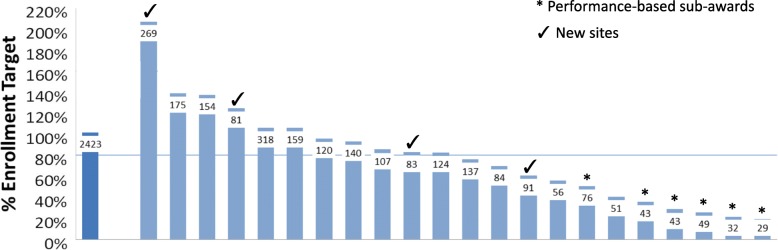
Results: Recruitment occurred from October 2013 through December 2016, requiring one additional year than the 2-year projection. Median enrollment at each site was 88 participants (range 29-318; 20 to 205% of the site target). At the end of year 1, study-wide recruitment was at 12% of the target (vs. 50% projected) and 12% of the total grant award was invested. The model constantly evaluated sites' needs and re-allocated resources to meet the study enrollment goal. If D2d had issued cost reimbursement subaward agreements and sites invoiced for their entire budget, 83% of the award would have been spent for all study activities over the first 4 years of the trial compared to 65% of the award spent (US$26M) under the hybrid model used by D2d.
Conclusions: It is feasible to foster a hybrid financial management approach to steward limited available public funds for research in a dynamic and consistent way that does not compromise the trial's scientific integrity and ensures conservation of funds to complete recruitment and continue to follow up participants.
Keywords: Budget; Clinical trial; Diabetes; Financial management; Hybrid; National Institutes of Health.
Conflict of interest statement
Ethics approval and consent to participate
The study is approved and monitored by an independent data and safety monitoring board (appointed by the National Institute of Diabetes and Digestive and Kidney Diseases) and the institutional review board of each collaborating clinical research site. Written informed consent was obtained from each participant prior to study procedures.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Battelle Technology Partnership Practice. Biopharmaceutical industry-sponsored clinical trials: impact on state economies. 2015. http://phrma-docs.phrma.org/sites/default/files/pdf/biopharmaceutical-in....
-
- Johnson J. Brief history of NIH funding: fact sheet. Congressional Research Service. Prepared for Members and Committes of Congress. 2013. https://www.everycrsreport.com/files/20131223_R43341_73c480e1172aef191e8....
-
- Reardon S, Tollefson J, Witze A, Ross E. US science agencies face deep cuts in Trump budget. 2017. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
