

Ankle and foot power in gait analysis: Implications for science, technology and clinical assessment
- PMID: 29724536
- PMCID: PMC6005760
- DOI: 10.1016/j.jbiomech.2018.04.017
Ankle and foot power in gait analysis: Implications for science, technology and clinical assessment
Abstract
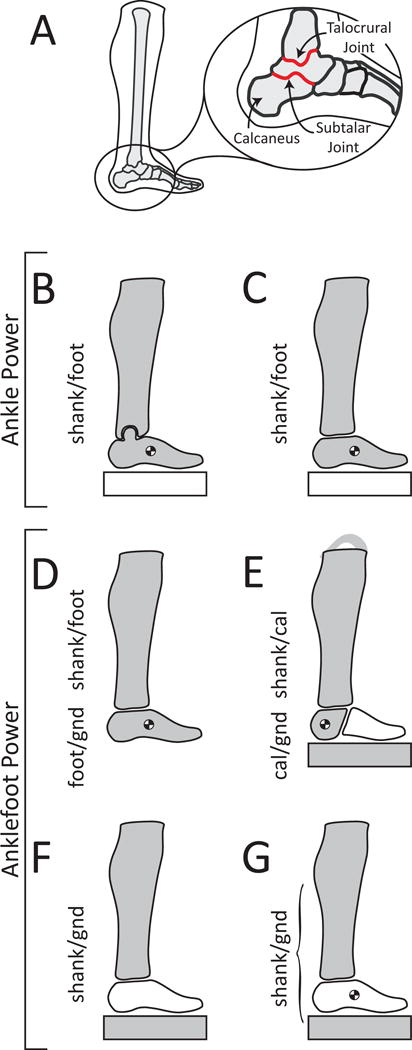
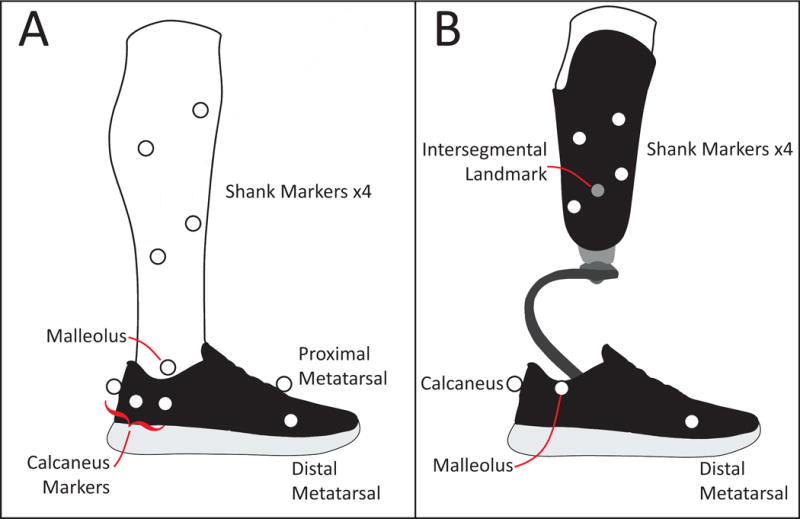
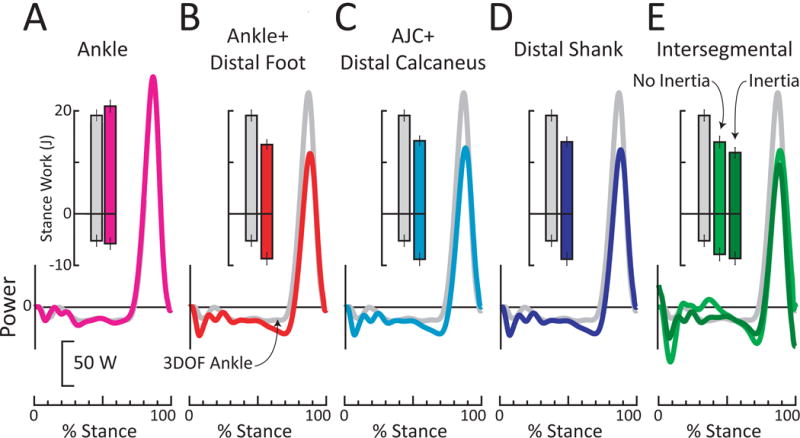
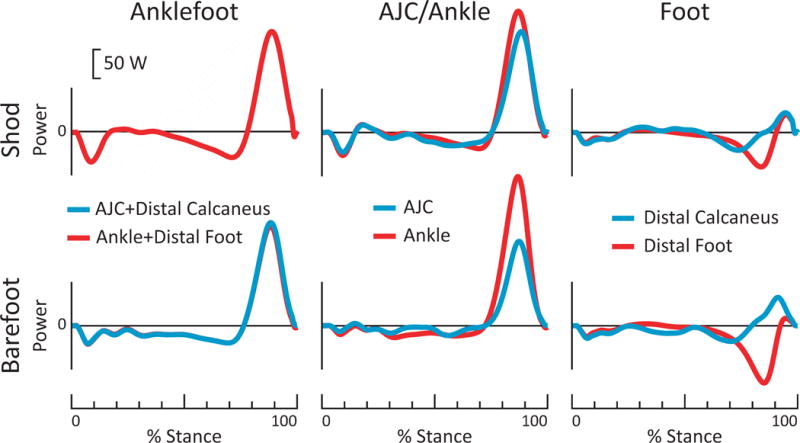
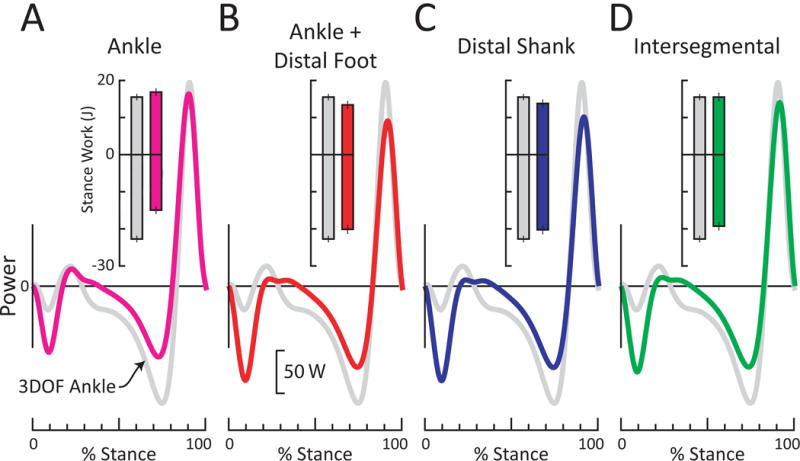
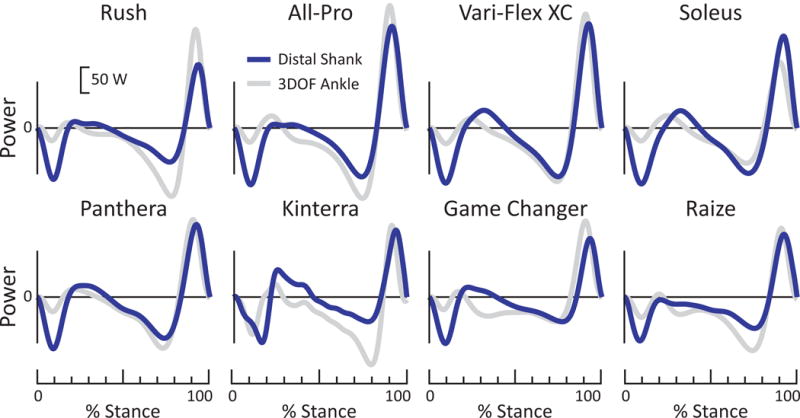
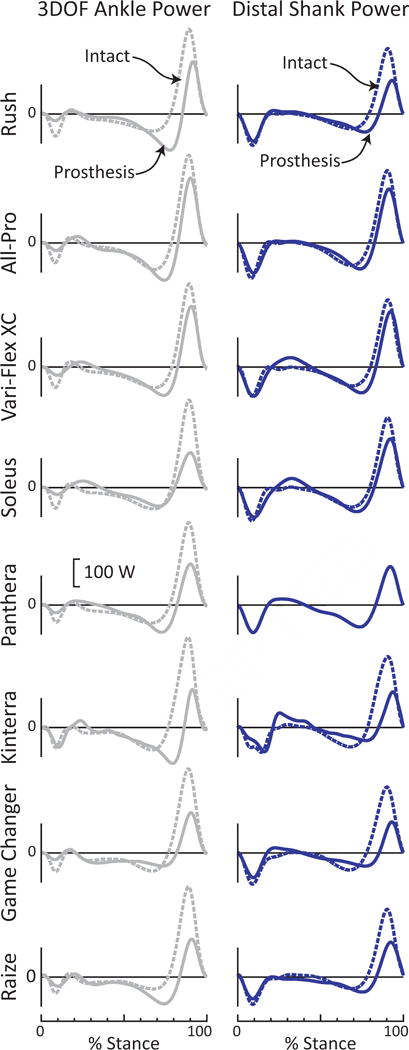
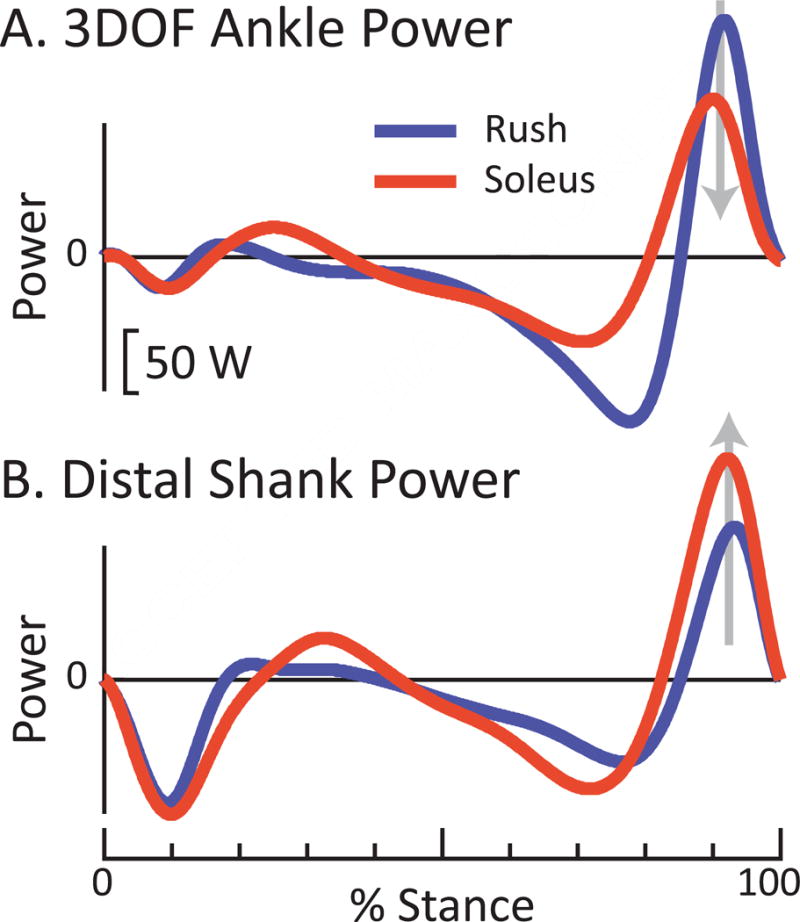
In human gait analysis studies, the entire foot is typically modeled as a single rigid-body segment; however, this neglects power generated/absorbed within the foot. Here we show how treating the entire foot as a rigid body can lead to misunderstandings related to (biological and prosthetic) foot function, and distort our understanding of ankle and muscle-tendon dynamics. We overview various (unconventional) inverse dynamics methods for estimating foot power, partitioning ankle vs. foot contributions, and computing combined anklefoot power. We present two case study examples. The first exemplifies how modeling the foot as a single rigid-body segment causes us to overestimate (and overvalue) muscle-tendon power generated about the biological ankle (in this study by up to 77%), and to misestimate (and misinform on) foot contributions; corroborating findings from previous multi-segment foot modeling studies. The second case study involved an individual with transtibial amputation walking on 8 different prosthetic feet. The results exemplify how assuming a rigid foot can skew comparisons between biological and prosthetic limbs, and lead to incorrect conclusions when comparing different prostheses/interventions. Based on analytical derivations, empirical findings and prior literature we recommend against computing conventional ankle power (between shank-foot). Instead, we recommend using an alternative estimate of power generated about the ankle joint complex (between shank-calcaneus) in conjunction with an estimate of foot power (between calcaneus-ground); or using a combined anklefoot power calculation. We conclude that treating the entire foot as a rigid-body segment is often inappropriate and ill-advised. Including foot power in biomechanical gait analysis is necessary to enhance scientific conclusions, clinical evaluations and technology development.
Keywords: Ankle joint; Inverse dynamics; Mechanical power; Multi-segment foot; Prosthetic feet.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
References
-
- Adamczyk PG, Roland M, Hahn ME. Sensitivity of biomechanical outcomes to independent variations of hindfoot and forefoot stiffness in foot prostheses. Hum Mov Sci. 2017;54:154–171. https://doi.org/10.1016/j.humov.2017.04.005. - DOI - PMC - PubMed
-
- Antonsson EK, Mann RW. The frequency content of gait. J Biomech. 1985;18:39–47. - PubMed
-
- Arch ES, Fylstra BL. Combined Ankle–Foot Energetics are Conserved When Distal Foot Energy Absorption is Minimized. J Appl Biomech. 2016;32:571–577. https://doi.org/10.1123/jab.2016-0108. - DOI - PubMed
-
- Baker RW. Measuring Walking: A Handbook of Clinical Gait Analysis. Wiley; 2013.
-
- Bogey RA, Perry J, Gitter AJ. An EMG-to-force processing approach for determining ankle muscle forces during normal human gait. IEEE Trans Neural Syst Rehabil Eng. 2005;13:302–310. https://doi.org/10.1109/TNSRE.2005.851768. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
