

Role of the Apparent Diffusion Coefficient as a Predictor of Tumor Progression in Patients with Chordoma
- PMID: 29724767
- PMCID: PMC7655429
- DOI: 10.3174/ajnr.A5664
Role of the Apparent Diffusion Coefficient as a Predictor of Tumor Progression in Patients with Chordoma
Abstract
Background and purpose: Diffusion-weighted imaging may aid in distinguishing aggressive chordoma from nonaggressive chordoma. This study explores the prognostic role of the apparent diffusion coefficient in chordomas.
Materials and methods: Sixteen patients with residual or recurrent chordoma were divided postoperatively into those with an aggressive tumor, defined as a growing tumor having a doubling time of <1 year, and those with a nonaggressive tumor on follow-up MR images. The ability of the ADC to predict an aggressive tumor phenotype was investigated by receiver operating characteristic analysis. The prognostic role of ADC was assessed using a Kaplan-Meier curve with a log-rank test.
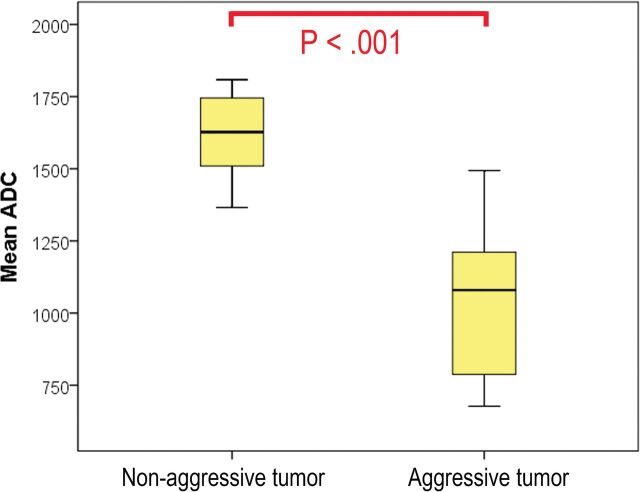
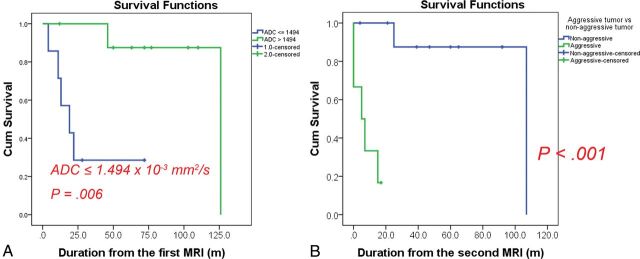
Results: Seven patients died during a median follow-up of 48 months (range, 4-126 months). Five of these 7 patients were in the aggressive tumor group, and 2 were in the nonaggressive tumor group. The mean ADC was significantly lower in the aggressive tumor group than in the nonaggressive tumor group (P = .002). Receiver operating characteristic analysis showed that a cutoff ADC value of 1.494 × 10-3 × mm2/s could be used to diagnose aggressive tumors with an area under the curve of 0.983 (95% CI, 0.911-1.000), a sensitivity of 1.000 (95% CI, 0.541-1.000), and a specificity of 0.900 (95% CI, 0.555-0.998). Furthermore, a cutoff ADC of ≤1.494 × 10-3 × mm2/s was associated with a significantly worse prognosis (P = .006).
Conclusions: Lower ADC values could predict tumor progression in postoperative chordomas.
© 2018 by American Journal of Neuroradiology.
Figures
References
-
- Fletcher CD, Bridge JA, Hogendoorn P, et al. . WHO Classification of Tumours of Soft Tissue and Bone. 4th ed Lyon: IARC Press; 2013
-
- Hanna SA, Tirabosco R, Amin A, et al. . Dedifferentiated chordoma: a report of four cases arising ‘de novo.’ J Bone Joint Surg Br 2008;90:652–56 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources