

The DOT1L inhibitor pinometostat reduces H3K79 methylation and has modest clinical activity in adult acute leukemia
- PMID: 29724899
- PMCID: PMC6265654
- DOI: 10.1182/blood-2017-12-818948
The DOT1L inhibitor pinometostat reduces H3K79 methylation and has modest clinical activity in adult acute leukemia
Abstract
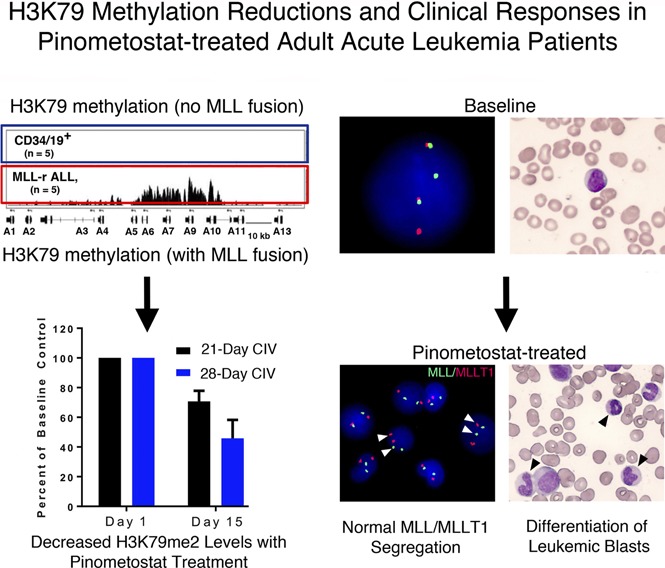
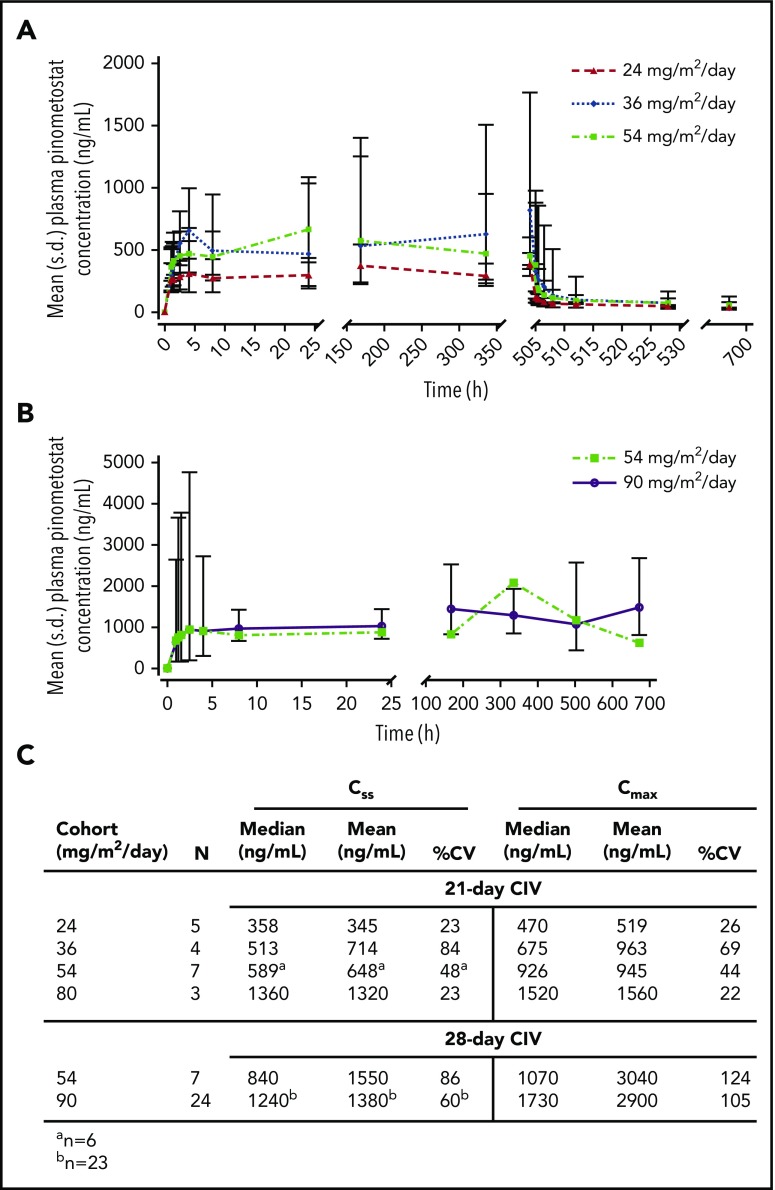
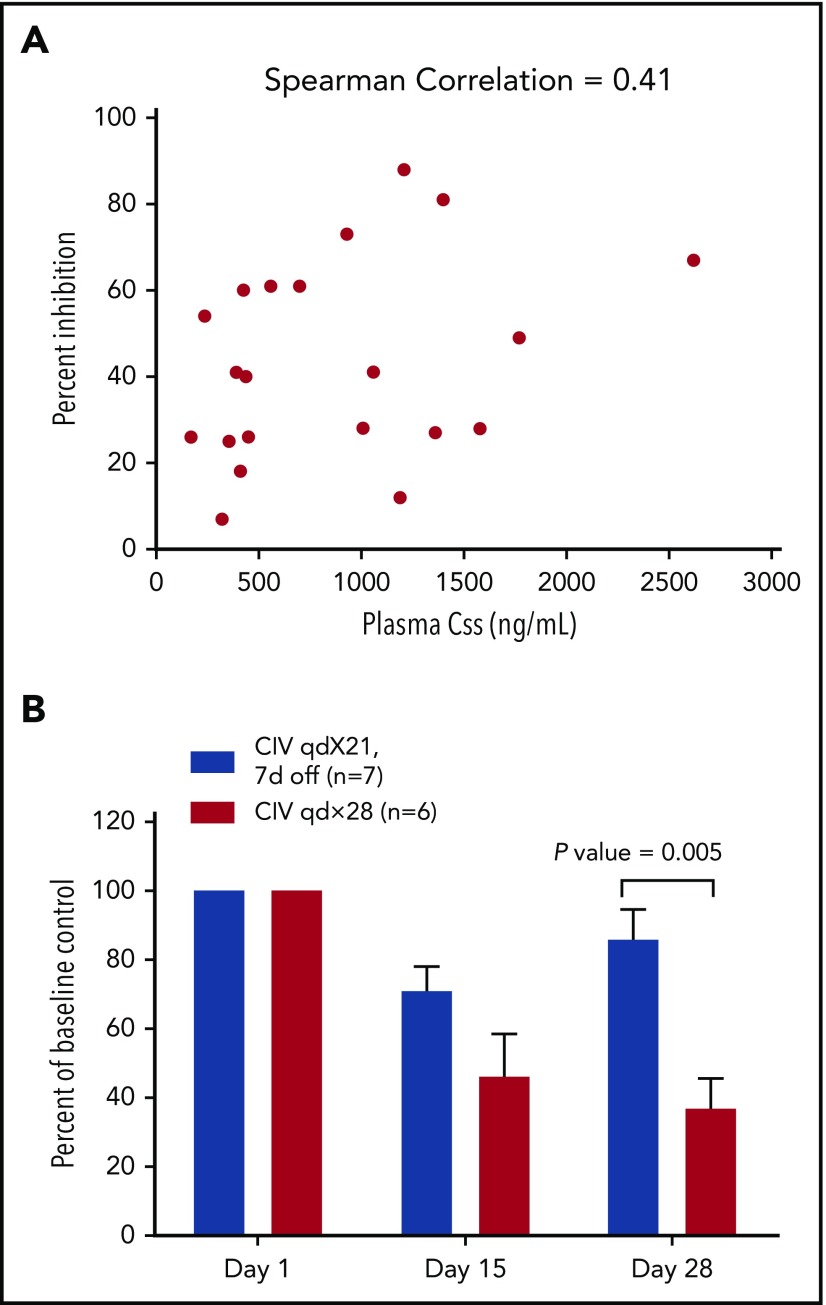
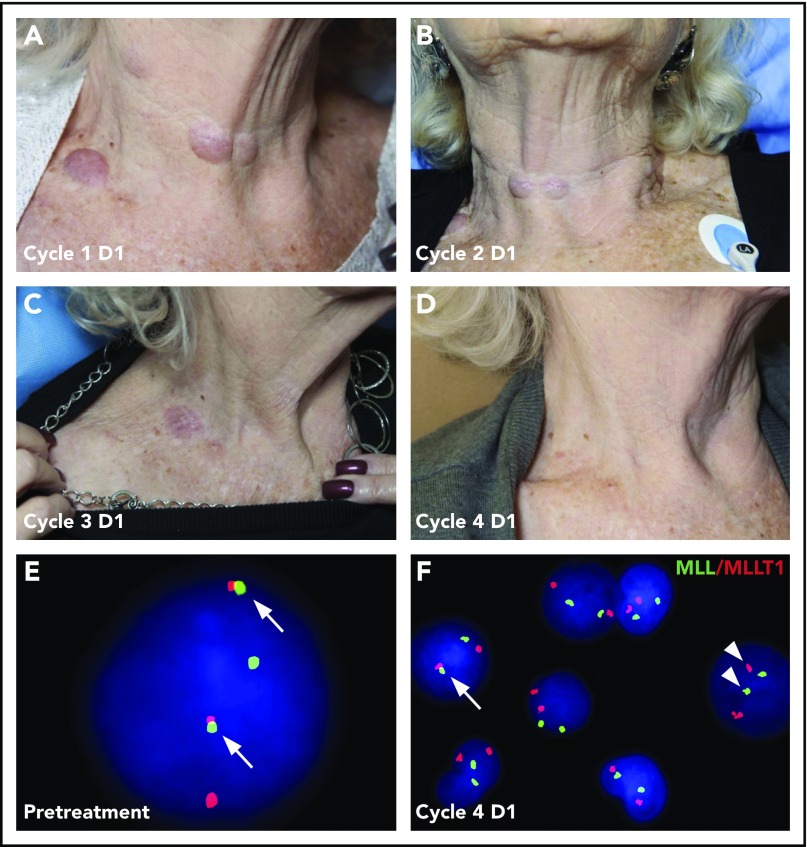
Pinometostat (EPZ-5676) is a first-in-class small-molecule inhibitor of the histone methyltransferase disrupter of telomeric silencing 1-like (DOT1L). In this phase 1 study, pinometostat was evaluated for safety and efficacy in adult patients with advanced acute leukemias, particularly those involving mixed lineage leukemia (MLL) gene rearrangements (MLL-r) resulting from 11q23 translocations. Fifty-one patients were enrolled into 6 dose-escalation cohorts (n = 26) and 2 expansion cohorts (n = 25) at pinometostat doses of 54 and 90 mg/m2 per day by continuous intravenous infusion in 28-day cycles. Because a maximum tolerated dose was not established in the dose-escalation phase, the expansion doses were selected based on safety and clinical response data combined with pharmacodynamic evidence of reduction in H3K79 methylation during dose escalation. Across all dose levels, plasma pinometostat concentrations increased in an approximately dose-proportional fashion, reaching an apparent steady-state by 4-8 hours after infusion, and rapidly decreased following treatment cessation. The most common adverse events, of any cause, were fatigue (39%), nausea (39%), constipation (35%), and febrile neutropenia (35%). Overall, 2 patients, both with t(11;19), experienced complete remission at 54 mg/m2 per day by continuous intravenous infusion, demonstrating proof of concept for delivering clinically meaningful responses through targeting DOT1L using the single agent pinometostat in MLL-r leukemia patients. Administration of pinometostat was generally safe, with the maximum tolerated dose not being reached, although efficacy as a single agent was modest. This study demonstrates the therapeutic potential for targeting DOT1L in MLL-r leukemia and lays the groundwork for future combination approaches in this patient population. This clinical trial is registered at www.clinicaltrials.gov as NCT01684150.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: E.M.S. received research funding and personal fees from Celgene Corporation and Agios Pharmaceuticals, Inc. R.T. received institutional research funding for trial participation. J.G.B. has received funding support from AbbVie, Amgen, Bluebird, Bristol-Myers Squibb, Celgene, Constellation, Curis, Janssen, Novartis, Takeda, Teva, and Vivolux. M.R.S. owns stock in Karyopharm Therapeutics; has a consulting/advisory role at Amgen, Astex, Celgene, Gilead, Incyte, Karyopharm Therapeutics, and TG Therapeutics; and receives research funding from Astex, Incyte, Sunesis, Takeda, and TG Therapeutics. J.K.A. has an advisory role at Immune Pharmaceuticals; received personal fees from and has an advisory role at Syros, Janssen Pharmaceuticals, Novartis, Bristol-Myers Squibb, Celgene, and Astellas; received institutional research funding for trial participation from Celgene, Astellas, Fujifilm, Genentech, ARIAD, Bayer, Celator, Cyclacel, Epizyme, Incyte, GlaxoSmithKline, Pfizer, Agios, and Boehringer Ingelheim; and received nonfinancial support from MC2. B.T., S.J.B., S.R.D., N.J.W., A.B.S., A.C., R.P., and E.H. are current or former employees of Epizyme and/or stockholders. S.A.A. is a consultant for Epizyme. J.D. is an employee and shareholder of Celgene. The remaining authors declare no competing financial interests.
Figures
References
-
- Schoch C, Schnittger S, Klaus M, Kern W, Hiddemann W, Haferlach T. AML with 11q23/MLL abnormalities as defined by the WHO classification: incidence, partner chromosomes, FAB subtype, age distribution, and prognostic impact in an unselected series of 1897 cytogenetically analyzed AML cases. Blood. 2003;102(7):2395-2402. - PubMed
-
- Garrido SM, Bryant E, Appelbaum FR. Allogeneic stem cell transplantation for relapsed and refractory acute myeloid leukemia patients with 11q23 abnormalities. Leuk Res. 2000;24(6):481-486. - PubMed
-
- Byrd JC, Mrózek K, Dodge RK, et al. ; Cancer and Leukemia Group B (CALGB 8461). Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461). Blood. 2002;100(13):4325-4336. - PubMed
-
- Krivtsov AV, Armstrong SA. MLL translocations, histone modifications and leukaemia stem-cell development. Nat Rev Cancer. 2007;7(11):823-833. - PubMed
-
- Felix CA. Secondary leukemias induced by topoisomerase-targeted drugs. Biochim Biophys Acta. 1998;1400(1-3):233-255. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
