

Transperitoneal Mini-Laparoscopic Pyeloplasty in Flank Position: A Safe Method for Infants and Young Adults
- PMID: 29725594
- PMCID: PMC5917372
- DOI: 10.3389/fsurg.2018.00032
Transperitoneal Mini-Laparoscopic Pyeloplasty in Flank Position: A Safe Method for Infants and Young Adults
Abstract
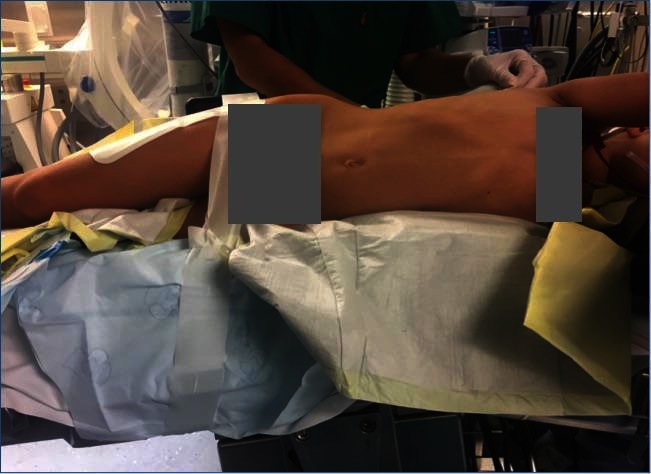
Introduction and objectives: Open dismembered pyeloplasty has been the gold standard treatment for ureteropelvic junction obstruction in children. Laparoscopic pyeloplasty (LP) is becoming a standard procedure, but its acceptance is slow. We report our method for minilaparoscopy (MLP) in children using a tansperitoneal approach with the patient in the lateral flank decubitus which we found technically advantageous.
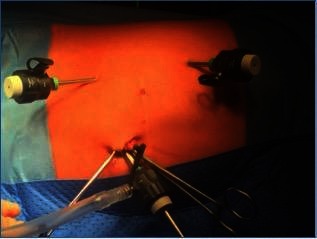
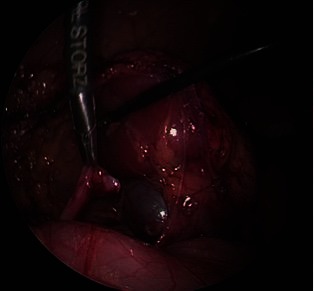
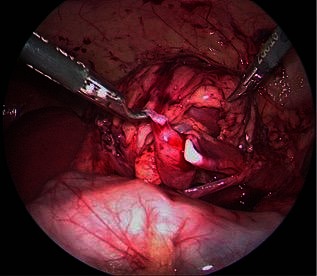
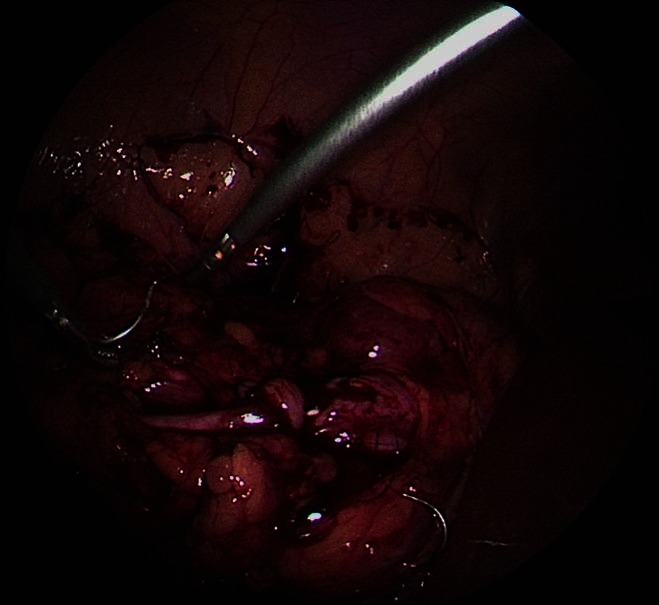
Materials and methods: Retrospective review of the records of 52 children and adolescents up to 18 years of age who underwent transperitoneal MLP at our institution during March 2012-October 2017 A 5 mm trocar is placed for the camera at the site of the umblicus by open technique, two 3 mm trocars placed in the upper and lower quadrants of the abdomen. No additional ports were necessary. 20cm long, 3-mm-diameter instruments are used. Few cases needed percutaneous fixation of the pelvis. The anastomosis is performed with 5-0 or 6-0 Polyglecaprone 25 (Monocryl®) with 13 mm half circle needle (TF plus) suture cut to 12-14 cm length and introduced through the 5-mm port. Needles are removed through the 3-mm port under direct vision.
Results: Fifty-two children (53 renal units) with a mean age of 82 months (range 3.5-204), a mean weight of 24,35 kg (range 7-57), and a mean follow-up of 20,44 months (6-60). Nine children were younger than 12 months, and 14 were ≤10kg. Six patients were >50kg. The mean of preoperative grade of dilatation was III (SFU scale) and postoperatively improved to SFU 0,60 (0-2). In 50 (94,3%) of the cases, there was complete resolution of hydronephrosis. There was no conversions to open surgery. Three patients suffered complications Clavien-Dindo Classification IIIb, 2 omental prolapses through a port site in two children which required general anaesthesia and one percutaneous drainage due to a leakage. No reinterventions related to stent complications or obstruction were found. Mean hospital stay was 4,69 (3-14) days.
Conclusions: The method of mini LP described here has proven efficient and safe. Weight appeared not to be limitation for both groups ≤10 and >50 kg.
Keywords: 3MM trocar; flank position; infants; laparoscopic pyeloplasty; laparoscopic pyeloplasty in children; short instruments.
Figures
References
-
- Tekgul S, Dogan HS, Erdem E, Hoebeke P, Kocvara R, Nijman JM, et al. Guidelines on paediatric urology. 2015 The Netherlands: European Association of Urology; (2015). http://uroweb.org/ individual-guidelines/non-oncology-guidelines/.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous