

Systematic Literature Review of Clinical and Economic Outcomes of Micro-Invasive Glaucoma Surgery (MIGS) in Primary Open-Angle Glaucoma
- PMID: 29725860
- PMCID: PMC5997597
- DOI: 10.1007/s40123-018-0131-0
Systematic Literature Review of Clinical and Economic Outcomes of Micro-Invasive Glaucoma Surgery (MIGS) in Primary Open-Angle Glaucoma
Abstract
Introduction: Primary open-angle glaucoma is estimated to affect 3% of the population aged 40-80 years. Trabeculectomy is considered the gold standard in surgical management of glaucoma; however, it is a technically complex procedure that may result in a range of adverse outcomes. Device-augmented, minimally invasive procedures (micro-invasive glaucoma surgeries, MIGS) have been developed aiming for safer and less invasive intraocular pressure (IOP) reduction compared with traditional surgery.
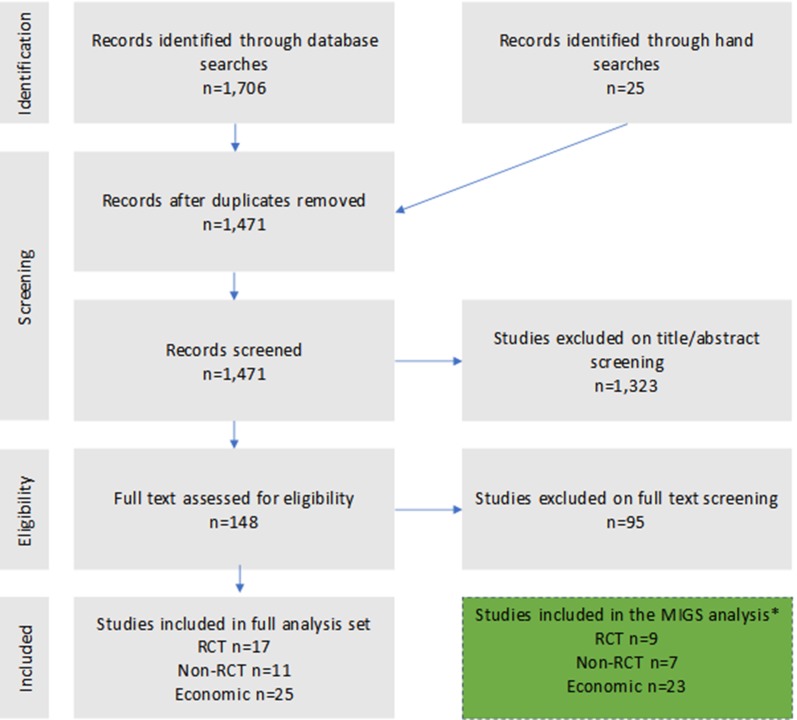
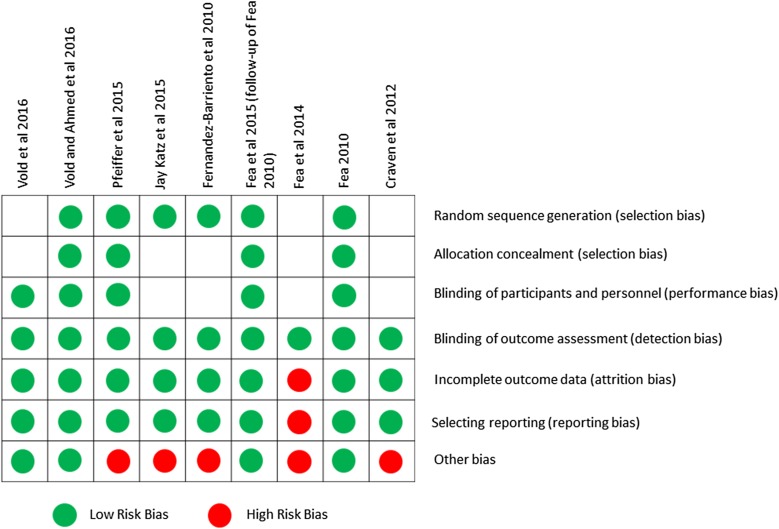
Methods: This paper presents results from a systematic literature review conducted in accordance with National Institute for Health and Care Excellence requirements for the Medical Technology Evaluation Programme via multiple databases from 2005 to 2016. For clinical outcomes, randomized clinical trials (RCTs) comparing MIGS with trabeculectomy or other therapies, observational studies, and other non-RCTs were included. Clinical outcomes reviewed were the change from baseline in mean IOP levels and change in topical glaucoma medication. Safety was assessed by reported harm and adverse events. For economic evidence, trials on cost-effectiveness, cost-utility, cost-benefit, cost-consequences, cost-minimization, cost of illness, and specific procedure costs were included. Risk of bias was assessed for clinical studies using the Cochrane Risk of Bias tool.
Results: A total of nine RCTs (seven iStents®, one Hydrus®, and one CyPass®), seven non-RCTs (three iStent®, three CyPass®, and one Hydrus®), and 23 economic studies were analyzed. While various forms of trabeculectomy can achieve postoperative IOP of between 11.0 and 13.0 mmHg, MIGS devices described in this review were typically associated with higher postoperative IOP levels. In addition, MIGS devices may result in increased hypotony rates or bleb needling in subconjunctival placed devices, requiring additional medical resources to manage. There is limited available evidence on the cost-effectiveness of MIGS and therefore it remains unclear whether the cost of using MIGS is outweighed by cost savings through decreased medication and need for further interventions.
Conclusion: Larger randomized trials and real-world observational studies are needed for MIGS devices to better assess clinical and economic effectiveness. Given the shortage of published data and increasing use of such procedures, living systematic reviews may help to provide ongoing and timely evidence-based direction for clinicians and decision makers. This review highlights the current unmet need for treatments that are easy to implement and reduce long-term IOP levels without increasing postoperative aftercare and cost.
Funding: Santen GmbH, Germany.
Keywords: CyPass; Hydrus; Intraocular pressure (IOP); MIGS; Micro-invasive; Open-angle glaucoma; Trabeculectomy; XEN; iStent.
Figures
References
-
- Schmid Biggerstaff K. Primary open-angle glaucoma (POAG). http://emedicine.medscape.com/article/1206147-overview. Accessed 4 Aug 2017.
-
- EGS. European Glaucoma Society guidelines, 4th ed. EGS; 2014. http://www.eugs.org. Accessed Aug 2017.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
