

Clinical effectiveness of liraglutide vs basal insulin in a real-world setting: Evidence of improved glycaemic and weight control in obese people with type 2 diabetes
- PMID: 29726082
- PMCID: PMC6099315
- DOI: 10.1111/dom.13335
Clinical effectiveness of liraglutide vs basal insulin in a real-world setting: Evidence of improved glycaemic and weight control in obese people with type 2 diabetes
Abstract
Aims: To compare real-world antidiabetic treatment outcomes over 12 months in obese people with type 2 diabetes mellitus (T2DM) who previously received oral antidiabetic therapy and then initiated a first injectable therapy with liraglutide or basal insulin.
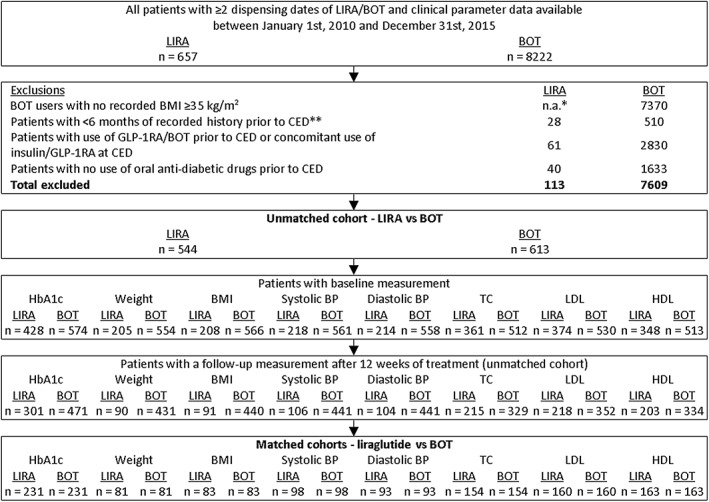
Patients and methods: This was a retrospective, propensity score-matched, longitudinal cohort study using real-world data (January 2010 to December 2015) from the Dutch PHARMO Database Network. Adult obese (body mass index [BMI] ≥35 kg/m2 ) patients with T2DM with ≥2 dispensing dates for liraglutide or basal insulin supported oral therapy (BOT) were selected. The primary endpoint was the change in glycated haemoglobin (HbA1c) from baseline during 12 months of follow-up. The secondary endpoints were the changes in weight, BMI and cardiovascular risk factors from baseline. Clinical data were analysed using descriptive statistics and compared using mixed models for repeated measures.
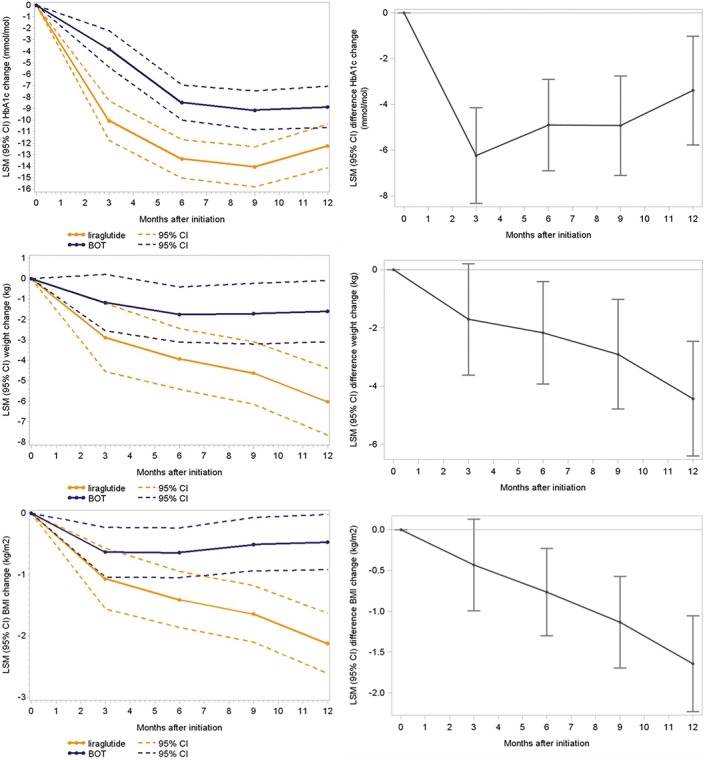
Results: Obese patients with T2DM (N = 1157) in each treatment group were matched (liraglutide cohort, n = 544; BOT cohort, n = 613). From 3 months onwards, glycaemic control improved in both cohorts but improved significantly more with liraglutide than with BOT (12 months: -12.2 mmol/mol vs -8.8 mmol/mol; P = .0053). In addition, weight and BMI were significantly lower for treatments with liraglutide vs BOT (12 months: -6.0 kg vs -1.6 kg and - 2.1 kg/m2 vs -0.5 kg/m2 , respectively; P < .0001 for both). No significant differences were seen in changes in cardiovascular risk factors.
Conclusions: The results of this real-world study in matched obese patients with T2DM showed that liraglutide was more effective than BOT for HbA1c control and weight/BMI reductions. Patients were more likely to maintain glycaemic control over time after initiating liraglutide than after initiating BOT.
Keywords: T2DM; liraglutide; obese; real-world data; the Netherlands.
© 2018 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
J.A.O., E.M.H., F.J.A.P. and R.M.C.H. are employees of the PHARMO Institute for Drug Outcomes Research. This independent research institute performs financially supported studies for government and related healthcare authorities, as well as for several pharmaceutical companies. E.L.H. and A.W.D. are employees of Novo Nordisk. C.K.T. is an employee of Novo Nordisk and owns stocks in Novo Nordisk A/S.
Figures
Similar articles
-
Efficacy and safety of liraglutide versus placebo added to basal insulin analogues (with or without metformin) in patients with type 2 diabetes: a randomized, placebo-controlled trial.Diabetes Obes Metab. 2015 Nov;17(11):1056-64. doi: 10.1111/dom.12539. Epub 2015 Sep 10. Diabetes Obes Metab. 2015. PMID: 26179619 Free PMC article. Clinical Trial.
-
The effects of GLP-1 analogues in obese, insulin-using type 2 diabetes in relation to eating behaviour.Int J Clin Pharm. 2016 Feb;38(1):144-51. doi: 10.1007/s11096-015-0219-8. Epub 2015 Nov 23. Int J Clin Pharm. 2016. PMID: 26597956 Free PMC article.
-
Liraglutide in people treated for type 2 diabetes with multiple daily insulin injections: randomised clinical trial (MDI Liraglutide trial).BMJ. 2015 Oct 28;351:h5364. doi: 10.1136/bmj.h5364. BMJ. 2015. PMID: 26512041 Free PMC article. Clinical Trial.
-
Improvement in glycated haemoglobin evaluated by baseline body mass index: a meta-analysis of the liraglutide phase III clinical trial programme.Diabetes Obes Metab. 2016 Jul;18(7):707-10. doi: 10.1111/dom.12617. Epub 2016 Feb 2. Diabetes Obes Metab. 2016. PMID: 26662611 Free PMC article. Review.
-
The Clinical Use of a Fixed-Dose Combination of Insulin Degludec and Liraglutide (Xultophy 100/3.6) for the Treatment of Type 2 Diabetes.Ann Pharmacother. 2018 Jan;52(1):69-77. doi: 10.1177/1060028017726348. Epub 2017 Aug 11. Ann Pharmacother. 2018. PMID: 28799414 Review.
Cited by
-
Clinical and economic outcomes among injection-naïve patients with type 2 diabetes initiating dulaglutide compared with basal insulin in a US real-world setting: the DISPEL Study.BMJ Open Diabetes Res Care. 2019 Dec 9;7(1):e000884. doi: 10.1136/bmjdrc-2019-000884. eCollection 2019. BMJ Open Diabetes Res Care. 2019. PMID: 31875137 Free PMC article.
-
Degree of obesity and gastrointestinal adverse reactions influence the weight loss effect of liraglutide in overweight or obese patients with type 2 diabetes.Ther Adv Chronic Dis. 2023 Mar 18;14:20406223231161516. doi: 10.1177/20406223231161516. eCollection 2023. Ther Adv Chronic Dis. 2023. PMID: 36950020 Free PMC article.
-
Liraglutide Effectiveness in Type 2 Diabetes: Insights from a Real-World Cohort of Portuguese Patients.Metabolites. 2022 Nov 16;12(11):1121. doi: 10.3390/metabo12111121. Metabolites. 2022. PMID: 36422260 Free PMC article.
-
Intensification of medical management in type 2 diabetes: A real-world look at primary care practice.J Diabetes Complications. 2020 Jan;34(1):107477. doi: 10.1016/j.jdiacomp.2019.107477. Epub 2019 Nov 6. J Diabetes Complications. 2020. PMID: 31711841 Free PMC article.
References
-
- Summers RH, Moore M, Byrne J, et al. Perceptions of weight, diabetes and willingness to participate in randomised controlled trials of bariatric surgery for patients with type 2 diabetes mellitus and body mass index 30‐39.9 kg/m(2). Obes Surg. 2015;25(6):1039‐1046. 10.1007/s11695-014-1479-4. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
