

Platelet Transfusion Practices in Critically Ill Children
- PMID: 29727368
- PMCID: PMC6476545
- DOI: 10.1097/CCM.0000000000003192
Platelet Transfusion Practices in Critically Ill Children
Abstract
Objectives: Little is known about platelet transfusions in pediatric critical illness. We sought to describe the epidemiology, indications, and outcomes of platelet transfusions among critically ill children.
Design: Prospective cohort study.
Setting: Multicenter (82 PICUs), international (16 countries) from September 2016 to April 2017.
Patients: Children ages 3 days to 16 years prescribed a platelet transfusion in the ICU during screening days.
Interventions: None.
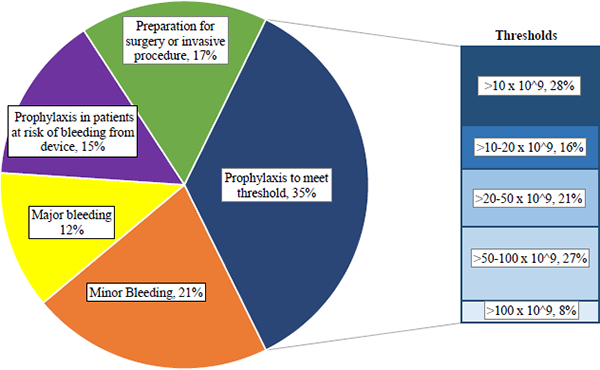
Measurements and main results: Over 6 weeks, 16,934 patients were eligible, and 559 received at least one platelet transfusion (prevalence, 3.3%). The indications for transfusion included prophylaxis (67%), minor bleeding (21%), and major bleeding (12%). Thirty-four percent of prophylactic platelet transfusions were prescribed when the platelet count was greater than or equal to 50 × 10 cells/L. The median (interquartile range) change in platelet count post transfusion was 48 × 10 cells/L (17-82 × 10 cells/L) for major bleeding, 42 × 10 cells/L (16-80 × 10 cells/L) for prophylactic transfusions to meet a defined threshold, 38 × 10 cells/L (17-72 × 10 cells/L) for minor bleeding, and 25 × 10 cells/L (10-47 × 10 cells/L) for prophylaxis in patients at risk of bleeding from a device. Overall ICU mortality was 25% but varied from 18% to 35% based on indication for transfusion. Upon adjusted analysis, total administered platelet dose was independently associated with increased ICU mortality (odds ratio for each additional 1 mL/kg platelets transfused, 1.002; 95% CI, 1.001-1.003; p = 0.005).
Conclusions: The majority of platelet transfusions are given as prophylaxis to nonbleeding children, and significant variation in platelet thresholds exists. Studies are needed to clarify appropriate indications, with focus on prophylactic transfusions.
Conflict of interest statement
Conflicts of Interest and Source of Funding: There are no conflicts of interest to disclose. This project was supported in part by funds from the Clinical Translational Science Center (CTSC), National Center for Advancing Translational Sciences (NCATS) grant #UL1-TR000457.
Figures

References
-
- Josephson C, Meyer E. Neonatal and pediatric transfusion practice In: AABB Technical Manual. Fung MK (ed). 18th edition Bethesda, MD, AABB, 2014, pp 571–597.
-
- Karam O, Demaret P, Shefler A, et al. Indications and Effects of Plasma Transfusions in Critically Ill Children. Am J Respir Crit Care Med. 2015. June 15; 191(12):1395–402. - PubMed
-
- Leteutre S, Duhamel A, Salleron J, et al. PELOD-2: an update of the Pediatric Logistic Organ Dysfunction score. Crit Care Med 2013; 41:1761–1773. - PubMed
-
- Stanworth SJ, Walsh TS, Prescott RJ, et al. Thrombocytopenia and platelet transfusion in UK critical care: a multicenter observational study. Transfusion 2013; 53:1050–1058. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
