

Mortality Measures to Profile Hospital Performance for Patients With Septic Shock
- PMID: 29727371
- PMCID: PMC6045435
- DOI: 10.1097/CCM.0000000000003184
Mortality Measures to Profile Hospital Performance for Patients With Septic Shock
Abstract
Objectives: Sepsis care is becoming a more common target for hospital performance measurement, but few studies have evaluated the acceptability of sepsis or septic shock mortality as a potential performance measure. In the absence of a gold standard to identify septic shock in claims data, we assessed agreement and stability of hospital mortality performance under different case definitions.
Design: Retrospective cohort study.
Setting: U.S. acute care hospitals.
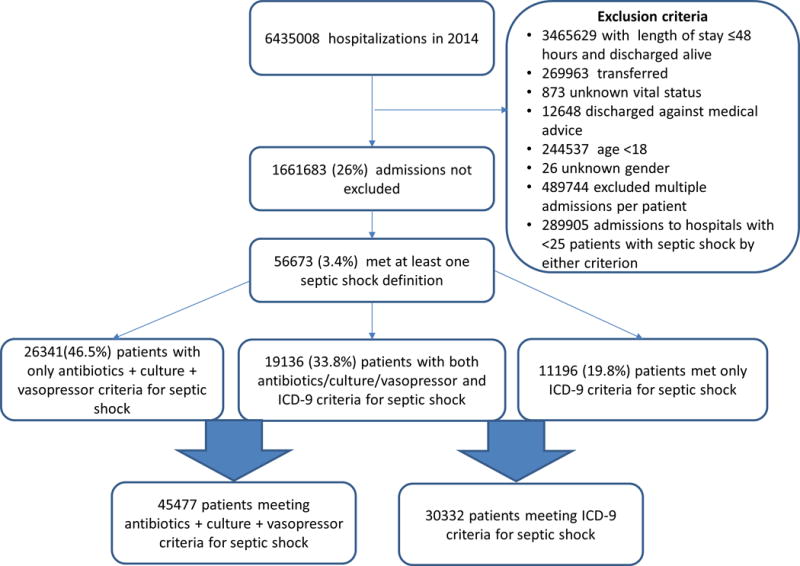
Patients: Hospitalized with septic shock at admission, identified by either implicit diagnosis criteria (charges for antibiotics, cultures, and vasopressors) or by explicit International Classification of Diseases, 9th revision, codes.
Interventions: None.
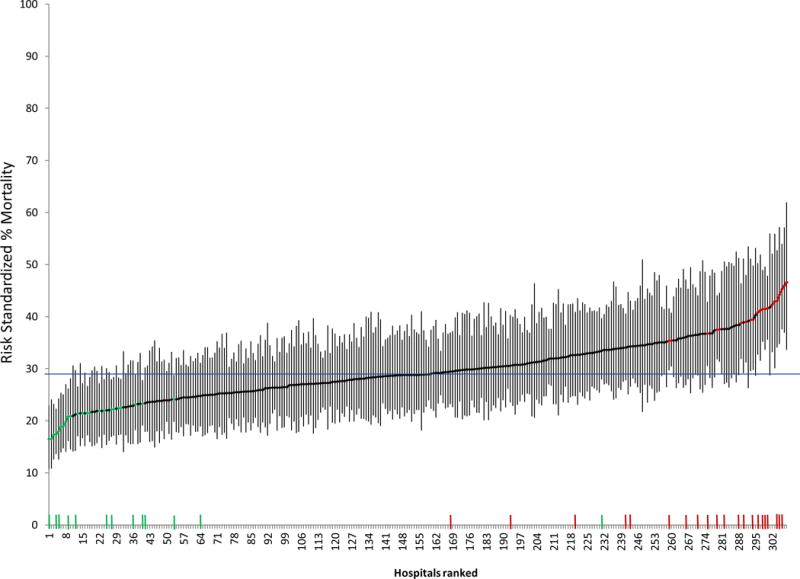
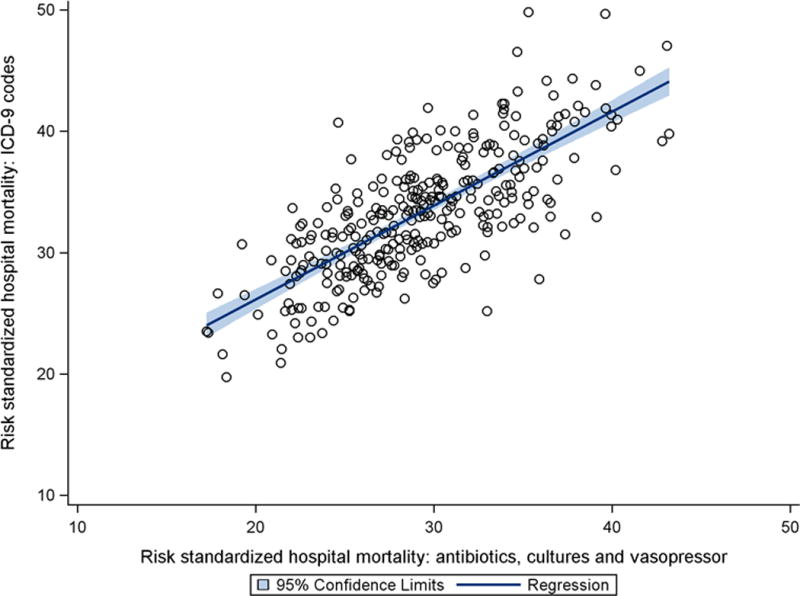
Measurements and main results: We used hierarchical logistic regression models to determine hospital risk-standardized mortality rates and hospital performance outliers. We assessed agreement in hospital mortality rankings when septic shock cases were identified by either explicit International Classification of Diseases, 9th revision, codes or implicit diagnosis criteria. Kappa statistics and intraclass correlation coefficients were used to assess agreement in hospital risk-standardized mortality and hospital outlier status, respectively. Fifty-six thousand six-hundred seventy-three patients in 308 hospitals fulfilled at least one case definition for septic shock, whereas 19,136 (33.8%) met both the explicit International Classification of Diseases, 9th revision, and implicit septic shock definition. Hospitals varied widely in risk-standardized septic shock mortality (interquartile range of implicit diagnosis mortality: 25.4-33.5%; International Classification of Diseases, 9th revision, diagnosis: 30.2-38.0%). The median absolute difference in hospital ranking between septic shock cohorts defined by International Classification of Diseases, 9th revision, versus implicit criteria was 37 places (interquartile range, 16-70), with an intraclass correlation coefficient of 0.72, p value of less than 0.001; agreement between case definitions for identification of outlier hospitals was moderate (kappa, 0.44 [95% CI, 0.30-0.58]).
Conclusions: Risk-standardized septic shock mortality rates varied considerably between hospitals, suggesting that septic shock is an important performance target. However, efforts to profile hospital performance were sensitive to septic shock case definitions, suggesting that septic shock mortality is not currently ready for widespread use as a hospital quality measure.
Conflict of interest statement
Dr. Shieh has disclosed that he does not have any potential conflicts of interest.
Figures
Comment in
-
Sepsis Redefined…Again.Crit Care Med. 2018 Aug;46(8):1378. doi: 10.1097/CCM.0000000000003230. Crit Care Med. 2018. PMID: 30004970 No abstract available.
References
-
- Elixhauser A, Friedman B, Stranges E. In: Septicemia in US hospitals, 2009. HCUP Agency for Healthcare Research and Quality, editor. Rockville, MD: 2011. - PubMed
-
- Mayr FB, Talisa VB, Balakumar V, et al. Proportion and cost of unplanned 30-day readmissions after sepsis compared with other medical conditions. JAMA. 2017 - PubMed
-
- PRISM Investigators. Early, goal-directed therapy for septic shock – A patient-level meta-analysis. N Engl J Med. 2017 - PubMed
-
- Marik PE, Linde-Zwirble WT, Bittner EA, et al. Fluid administration in severe sepsis and septic shock, patterns and outcomes: An analysis of a large national database. Intensive Care Med. 2017;43:625–632. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
