

Development and validation of a pre-hospital "Red Flag" alert for activation of intra-hospital haemorrhage control response in blunt trauma
- PMID: 29728151
- PMCID: PMC5935988
- DOI: 10.1186/s13054-018-2026-9
Development and validation of a pre-hospital "Red Flag" alert for activation of intra-hospital haemorrhage control response in blunt trauma
Abstract
Background: Haemorrhagic shock is the leading cause of early preventable death in severe trauma. Delayed treatment is a recognized prognostic factor that can be prevented by efficient organization of care. This study aimed to develop and validate Red Flag, a binary alert identifying blunt trauma patients with high risk of severe haemorrhage (SH), to be used by the pre-hospital trauma team in order to trigger an adequate intra-hospital standardized haemorrhage control response: massive transfusion protocol and/or immediate haemostatic procedures.
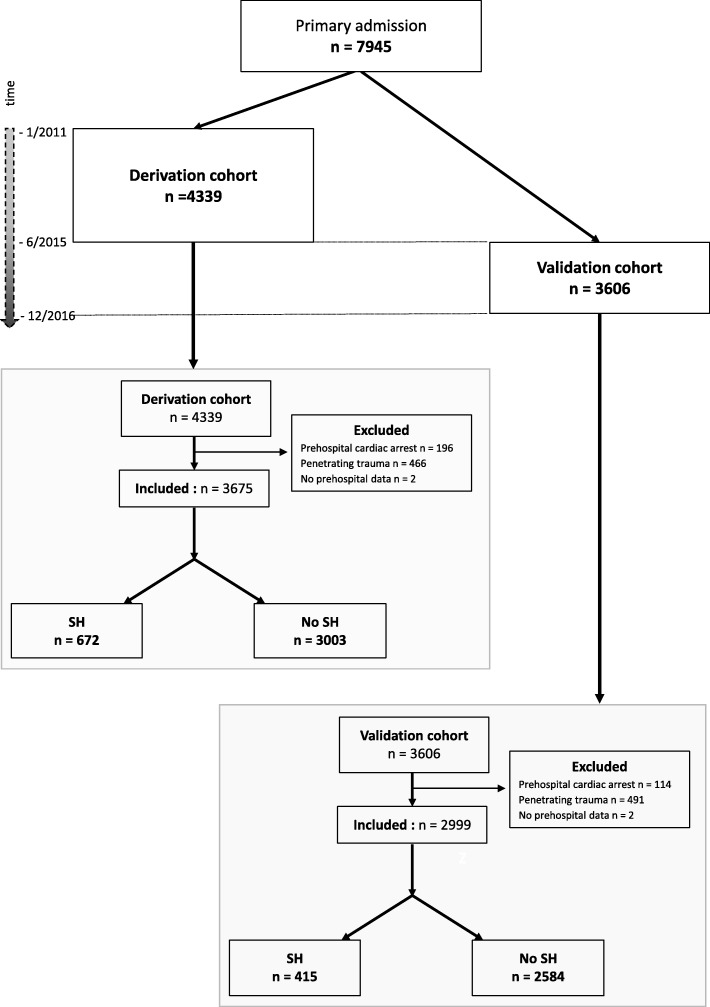
Methods: A multicentre retrospective study of prospectively collected data from a trauma registry (Traumabase®) was performed. SH was defined as: packed red blood cell (RBC) transfusion in the trauma room, or transfusion ≥ 4 RBC in the first 6 h, or lactate ≥ 5 mmol/L, or immediate haemostatic surgery, or interventional radiology and/or death of haemorrhagic shock. Pre-hospital characteristics were selected using a multiple logistic regression model in a derivation cohort to develop a Red Flag binary alert whose performances were confirmed in a validation cohort.
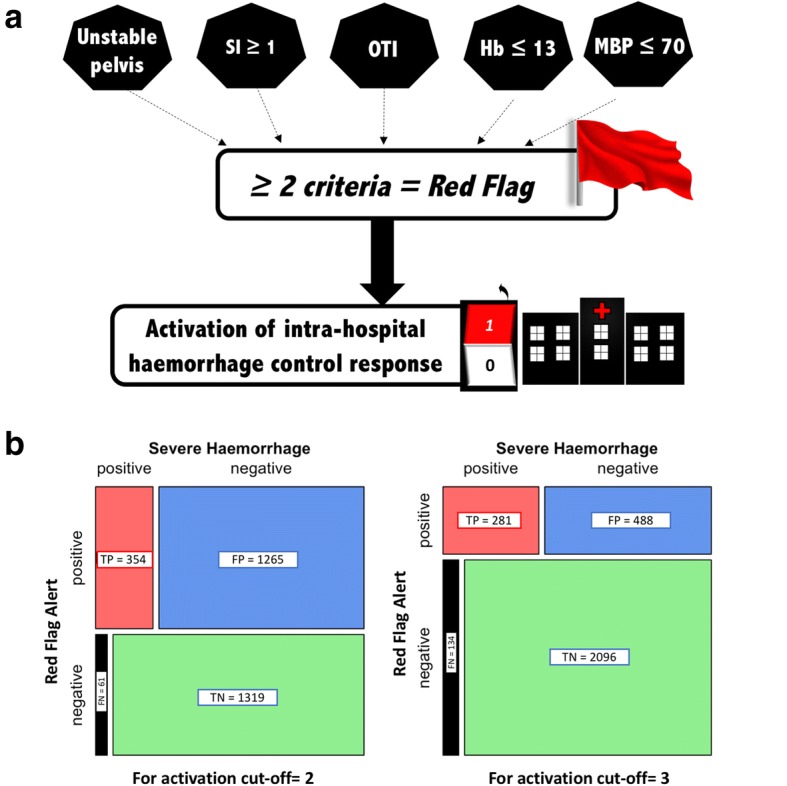
Results: Among the 3675 patients of the derivation cohort, 672 (18%) had SH. The final prediction model included five pre-hospital variables: Shock Index ≥ 1, mean arterial blood pressure ≤ 70 mmHg, point of care haemoglobin ≤ 13 g/dl, unstable pelvis and pre-hospital intubation. The Red Flag alert was triggered by the presence of any combination of at least two criteria. Its predictive performances were sensitivity 75% (72-79%), specificity 79% (77-80%) and area under the receiver operating characteristic curve 0.83 (0.81-0.84) in the derivation cohort, and were not significantly different in the independent validation cohort of 2999 patients.
Conclusion: The Red Flag alert developed and validated in this study has high performance to accurately predict or exclude SH.
Keywords: Anticipation; Organization; Protocol; Severe haemorrhage; Severe trauma.
Conflict of interest statement
Ethics approval and consent to participate
The data come from the Traumabase®. This registry obtained approval from the Advisory Committee for Information Processing in Health Research (CCTIRS, 11.305bis) and from the National Commission on Informatics and Liberties (CNIL, 911461), and the analysis meets the requirement of the local and national ethics committee (Comité de Protection des Personnes, Paris VI).
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
