

C3 glomerulopathy associated with monoclonal Ig is a distinct subtype
- PMID: 29729982
- PMCID: PMC7735221
- DOI: 10.1016/j.kint.2018.01.037
C3 glomerulopathy associated with monoclonal Ig is a distinct subtype
Erratum in
-
Ravindran A, Fervenza FC, Smith RJH, Sethi S. C3 glomerulopathy associated with monoclonal Ig is a distinct subtype. Kidney Int. 2018;94:178-186.Kidney Int. 2018 Nov;94(5):1025. doi: 10.1016/j.kint.2018.08.001. Kidney Int. 2018. PMID: 30348291 No abstract available.
Abstract
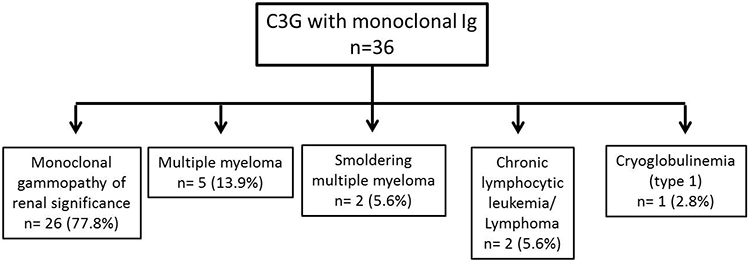
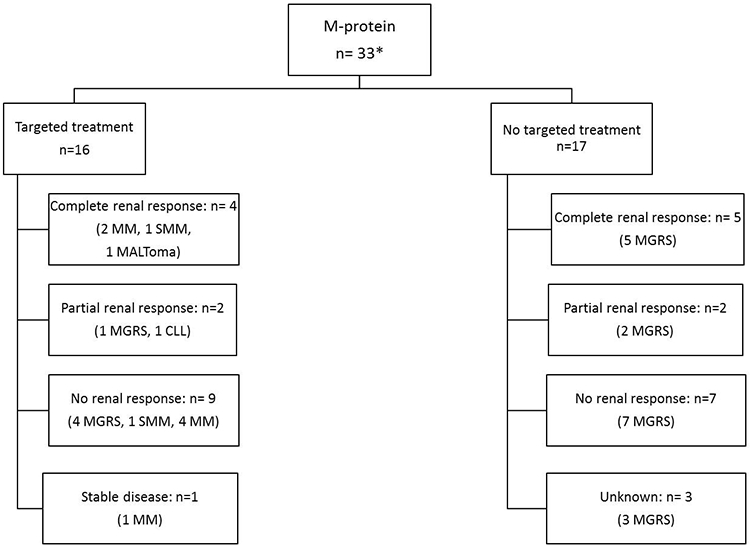
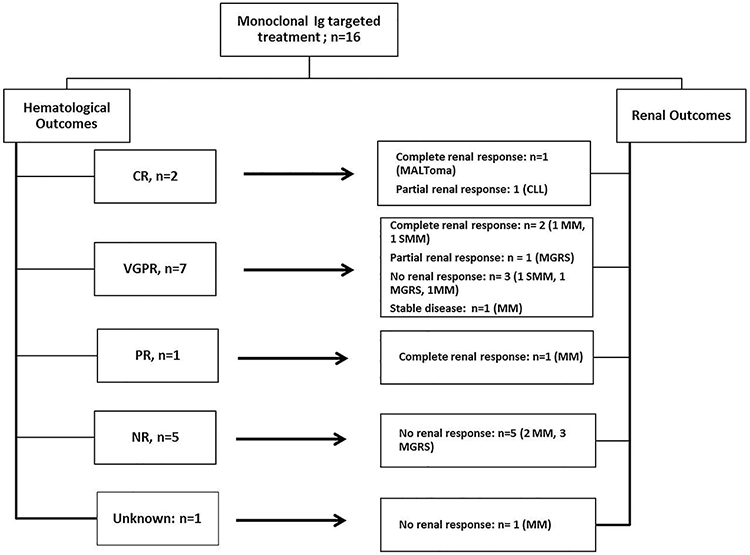
Monoclonal immunoglobulins (MIg) may play a causal role in C3 glomerulopathy (C3G) by impairing regulation of the alternative pathway of complement. Ninety-five patients with C3G were tested for MIg of which 36 were positive. Their mean age at diagnosis was 60 years and among patient 50 years and older, 65.1% had a MIg. At presentation, median serum creatinine and proteinuria were 1.9 mg/dL and 3.0 g/24 hours. Hematuria was present in 32 (88.9%) patients. Twelve (34.3%) patients had low C3 levels. C3 nephritic factor was detected in 45.8% patients; pathogenic variants in complement protein genes were rare. Hematologic evaluation revealed monoclonal gammopathy of renal significance in 26 patients, multiple myeloma in five, smoldering multiple myeloma in two, and chronic lymphocytic leukemia, lymphoma, or type I cryoglobulin each in one patient. After a median follow-up of 43.6 months, the median serum creatinine and proteinuria were 1.4 mg/dL and 0.8g/24 hours. Nine patients developed ESRD. Sixteen patients received MIg-targeted treatment, 17 patients received non-targeted treatment while three patients were managed conservatively. Of the 16 patients receiving MIg-targeted treatment, ten achieved complete/very good/partial hematologic response. Of these, seven achieved a complete/partial/stable renal response. Five patients receiving targeted treatment did not achieve hematologic response, none had a renal response. Patients receiving targeted treatment were more likely to have multiple myeloma/smoldering multiple myeloma. Patients receiving non-targeted treatment were more likely to have monoclonal gammopathy of renal significance. Thus, C3G with MIg is seen in older patients, C3 nephritic factor is the most common autoantibody detected, and MIg-targeted treatment may result in remission and stabilization of kidney function in a subset of these patients.
Keywords: C3 glomerulonephritis; C3 glomerulopathy; alternative pathway of complement; dense deposit disease; monoclonal Ig.
Copyright © 2018 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Conservative treatment for C3 glomerulopathy and monoclonal Ig.Kidney Int. 2018 Sep;94(3):632. doi: 10.1016/j.kint.2018.05.027. Kidney Int. 2018. PMID: 30143070 No abstract available.
-
The authors reply.Kidney Int. 2018 Sep;94(3):632-633. doi: 10.1016/j.kint.2018.06.002. Kidney Int. 2018. PMID: 30143071 No abstract available.
References
-
- Angioi A, Fervenza FC, Sethi S, et al. Diagnosis of complement alternative pathway disorders. Kidney International 2016;89:278–88. - PubMed
-
- Servais A, Noel L-H, Roumenina LT, et al. Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies. Kidney Int 2012;82:454–64. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
