

The Role of Osteotomy for the Treatment of PCL Injuries
- PMID: 29730857
- PMCID: PMC5970123
- DOI: 10.1007/s12178-018-9488-x
The Role of Osteotomy for the Treatment of PCL Injuries
Abstract
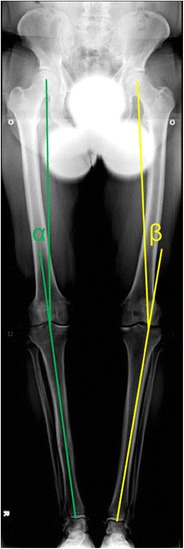
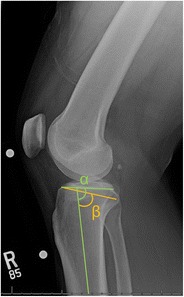
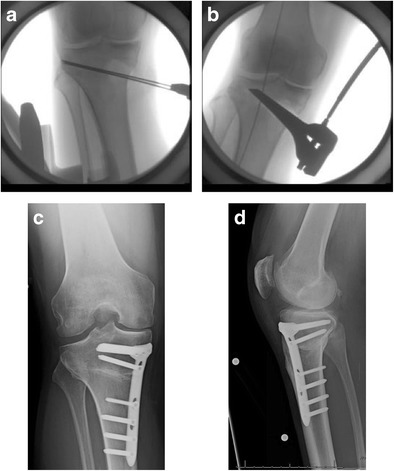
Purpose of review: The purposes of this review are to (1) describe the anatomic and biomechanical rationale for high tibial osteotomy (HTO) in the setting of posterior cruciate ligament (PCL) deficiency, (2) review the indications for concomitant HTO and PCL reconstruction, (3) provide guidance for the clinical assessment of the patient with suspected PCL deficiency, and (4) summarize the key surgical steps necessary to attain the appropriate sagittal and coronal plane corrections.
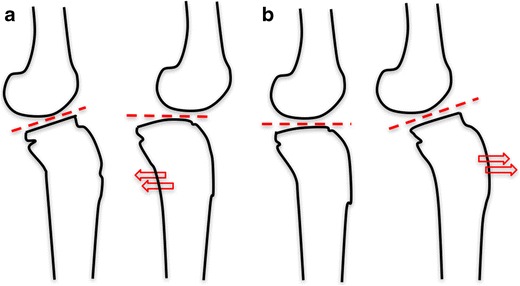
Recent findings: The preponderance of available biomechanical data pertaining to the PCL-deficient knee suggests that an increased proximal tibial slope limits posterior tibial translation under axial compressive loads. Moreover, recent clinical data has demonstrated that decreased proximal tibial slope may exacerbate residual anterior-posterior laxity and jeopardize the durability of PCL reconstruction. Thus, in the setting of PCL deficiency, an HTO that increases the posterior tibial slope may be advisable. HTO may be an important treatment adjunct in the surgical management of PCL deficiency. In the setting of chronic injuries and varus malalignment, HTO should be considered in order to ensure a durable ligamentous reconstruction and forestall the progression of secondary osteoarthritis.
Keywords: High tibial osteotomy (HTO); Posterior cruciate ligament (PCL); Posterior tibial translation; Tibial slope; Varus malalignment.
Conflict of interest statement
Conflict of Interest
All authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
