

Is the Isolated-Tip Needle-Knife Precut as Effective as Conventional Precut Fistulotomy in Difficult Biliary Cannulation?
- PMID: 29730907
- PMCID: PMC6143454
- DOI: 10.5009/gnl17572
Is the Isolated-Tip Needle-Knife Precut as Effective as Conventional Precut Fistulotomy in Difficult Biliary Cannulation?
Abstract
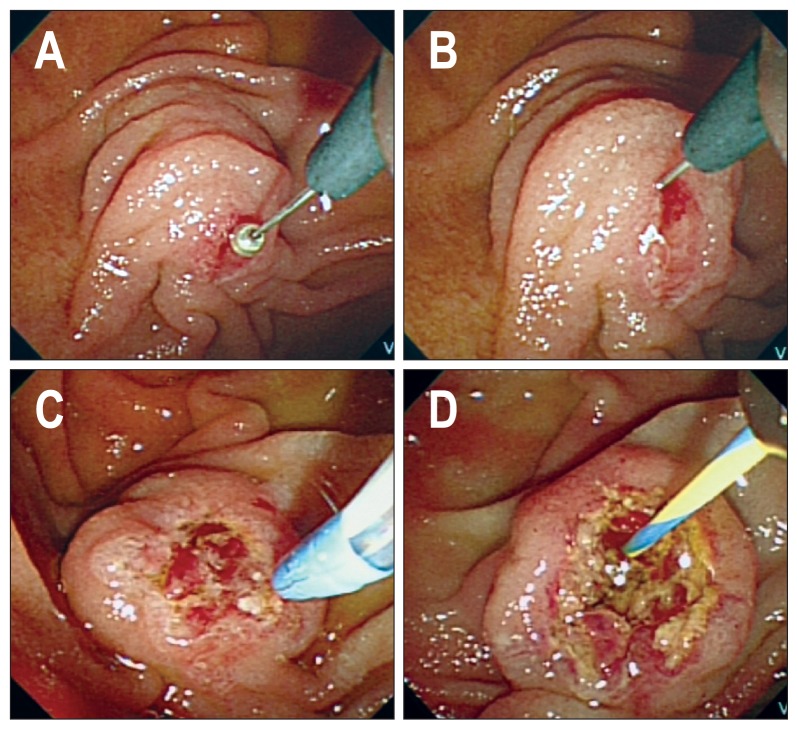
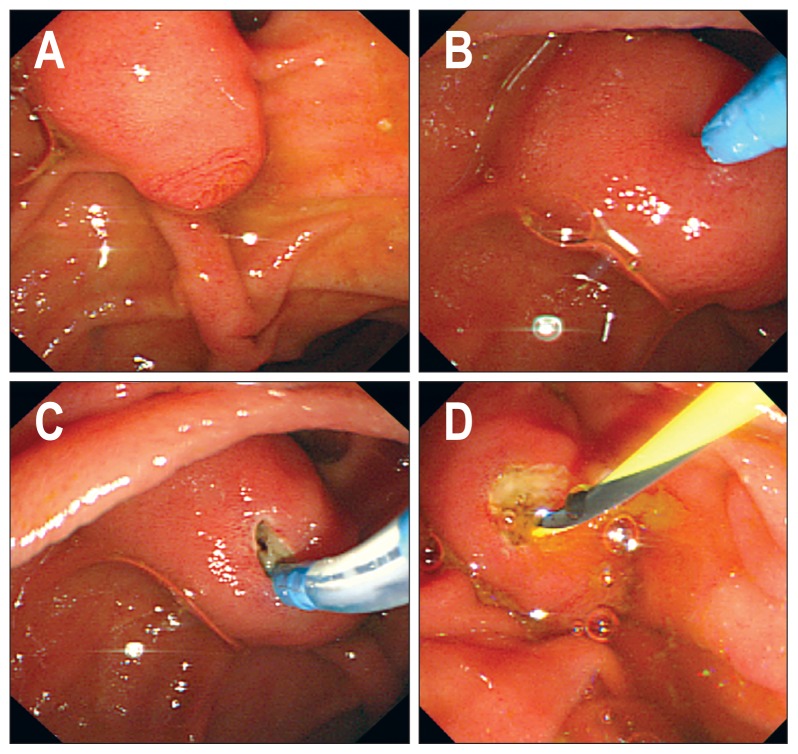
Background/aims: Needle-knife precut fistulotomy (NK-F) is a well-known freehand technique for difficult biliary cannulation (DBC). Another approach involves the use of Iso-Tome®, a modified precutting device with an insulated needle tip to prevent direct thermal injury. This comparative study aimed to evaluate the efficacy of the Iso-Tome® precut (IT-P) compared to that of NK-F for DBC.
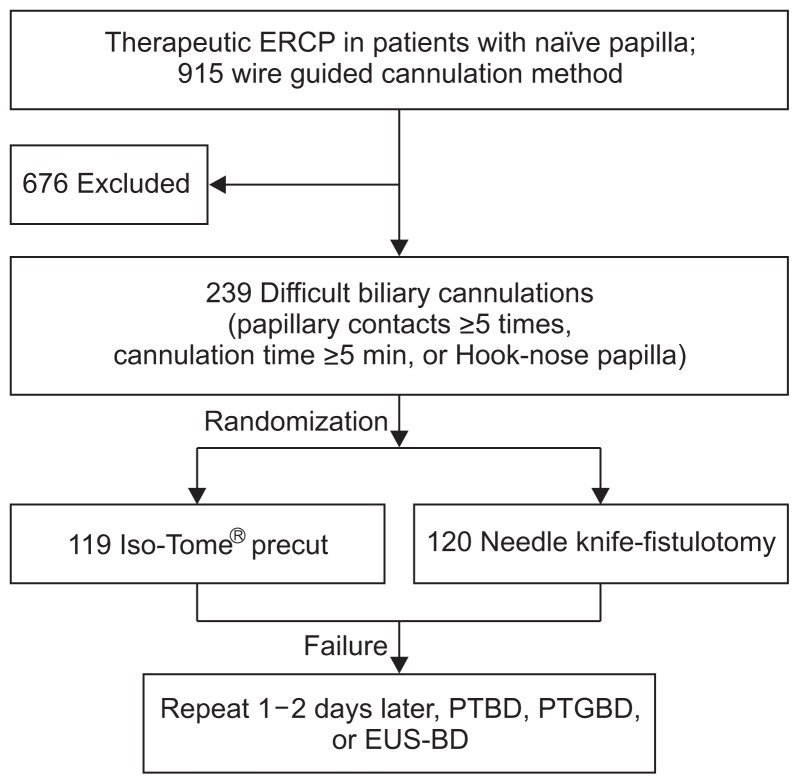
Methods: Patients with a naïve papilla who underwent early IT-P or NK-F for DBC were enrolled. DBC was defined as failure to achieve selective biliary access by wire-guided cannulation despite 5 minutes of attempted cannulation, ≥5 papillary contacts, or a hooknose-shaped papilla. The primary endpoint was the primary technical success rate, which was based on a noninferiority model.
Results: A total of 239 DBC cases were enrolled. The primary technical success rates were 74.7% (89/119) in the IT-P group and 91.6% (110/120) in the NK-F group (lower limit of 90% confidence interval, -0.23; p=0.927 for a noninferiority margin of 10%). The total technical success rates were 87.4% and 95.0%, respectively (p=0.038). The mean precutting times for successful biliary access were 11.2 minutes for IT-P and 7.3 minutes for NK-F (p<0.01). The procedure-related adverse event rates were 9.2% for IT-P and 5.8% for NK-F (p=0.318). The rates of post-endoscopic retrograde cholangiopancreatography pancreatitis were 4.2% and 2.5%, respectively (p=0.499).
Conclusions: IT-P failed to exhibit noninferiority compared with NK-F regarding the primary technical success rate of DBC, but there was no difference in the frequency of adverse events.
Keywords: Biliary; Cannulation; Iso-Tome; Needle-knife; Precut.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline.Endoscopy. 2016 Jul;48(7):657-83. doi: 10.1055/s-0042-108641. Epub 2016 Jun 14. Endoscopy. 2016. PMID: 27299638
-
Early precut fistulotomy for biliary access: time to change the paradigm of "the later, the better"?Gastrointest Endosc. 2014 Oct;80(4):634-641. doi: 10.1016/j.gie.2014.03.014. Epub 2014 May 6. Gastrointest Endosc. 2014. PMID: 24814775
-
Needle-knife precut papillotomy with a small incision over a pancreatic stent improves the success rate and reduces the complication rate in difficult biliary cannulations.J Hepatobiliary Pancreat Sci. 2013 Mar;20(3):382-8. doi: 10.1007/s00534-012-0552-4. J Hepatobiliary Pancreat Sci. 2013. PMID: 22993078
-
Transpancreatic Sphincterotomy Is Effective and Safe in Expert Hands on the Short Term.Dig Dis Sci. 2019 Sep;64(9):2429-2444. doi: 10.1007/s10620-019-05640-4. Epub 2019 May 4. Dig Dis Sci. 2019. PMID: 31055720 Free PMC article.
-
Biliary Cannulation in Endoscopic Retrograde Cholangiography: How to Tackle the Difficult Papilla.Dig Dis. 2022;40(1):85-96. doi: 10.1159/000515692. Epub 2021 Mar 8. Dig Dis. 2022. PMID: 33684915 Review.
Cited by
-
Meta-analysis of the effectiveness of early endoscopic treatment of Acute biliary pancreatitis based on lightweight deep learning model.BMC Gastroenterol. 2024 Aug 28;24(1):292. doi: 10.1186/s12876-024-03361-1. BMC Gastroenterol. 2024. PMID: 39198766 Free PMC article.
-
Primary needle-knife fistulotomy for preventing post-endoscopic retrograde cholangiopancreatography pancreatitis: Importance of the endoscopist's expertise level.World J Clin Cases. 2021 Jun 16;9(17):4166-4177. doi: 10.12998/wjcc.v9.i17.4166. World J Clin Cases. 2021. PMID: 34141779 Free PMC article.
-
Success and Safety of Needle Knife Papillotomy and Fistulotomy Based on Papillary Anatomy: A Prospective Controlled Trial.Dig Dis Sci. 2022 May;67(5):1901-1909. doi: 10.1007/s10620-021-06983-7. Epub 2021 Jun 3. Dig Dis Sci. 2022. PMID: 34081249 Clinical Trial.
-
Rescue cannulation techniques in difficult biliary access-A comprehensive review.Indian J Gastroenterol. 2025 Jun;44(3):286-297. doi: 10.1007/s12664-024-01718-8. Epub 2025 Feb 7. Indian J Gastroenterol. 2025. PMID: 39918679 Review.
-
Efficacy of a Newly Developed Guidewire for Selective Biliary Cannulation: A Multicenter Randomized Controlled Trial.J Clin Med. 2023 May 12;12(10):3440. doi: 10.3390/jcm12103440. J Clin Med. 2023. PMID: 37240546 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
