

Electrophysiologic Characterization of Calcium Handling in Human Induced Pluripotent Stem Cell-Derived Atrial Cardiomyocytes
- PMID: 29731429
- PMCID: PMC5989733
- DOI: 10.1016/j.stemcr.2018.04.005
Electrophysiologic Characterization of Calcium Handling in Human Induced Pluripotent Stem Cell-Derived Atrial Cardiomyocytes
Abstract
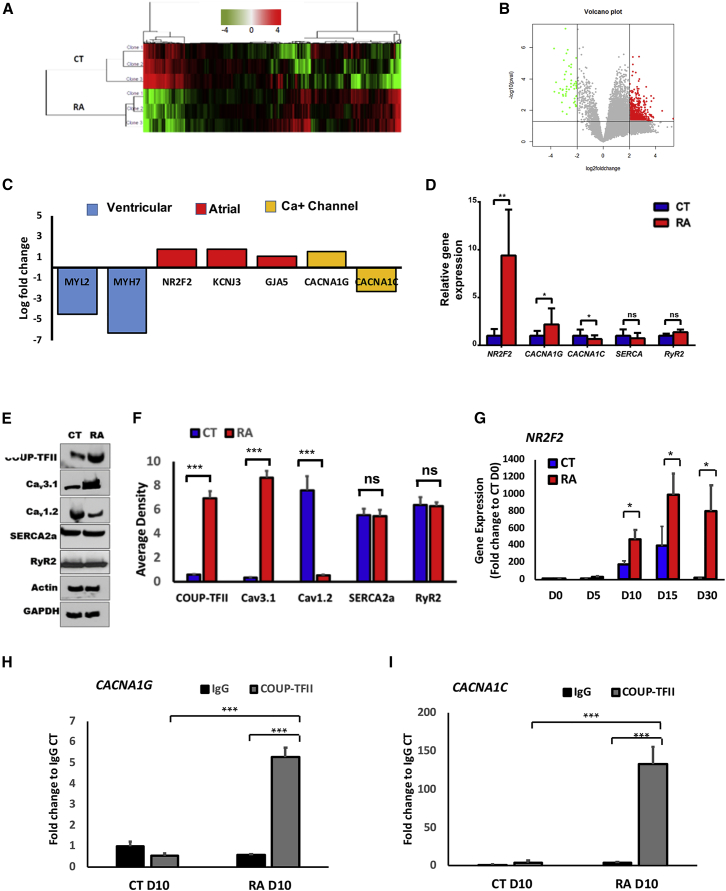
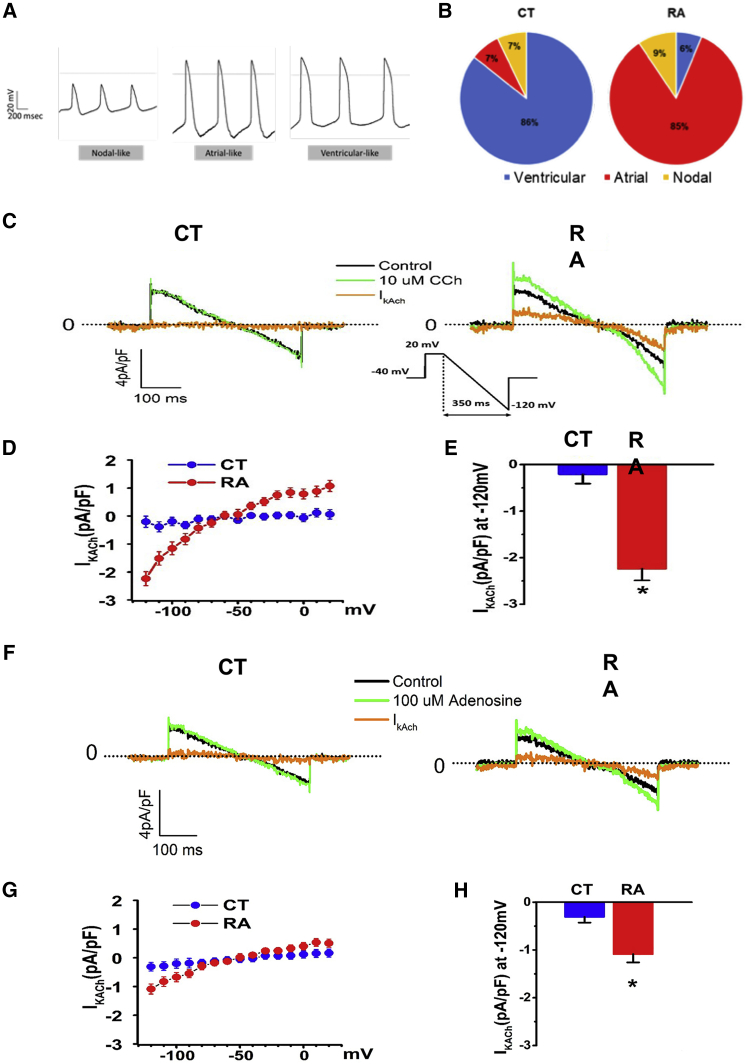
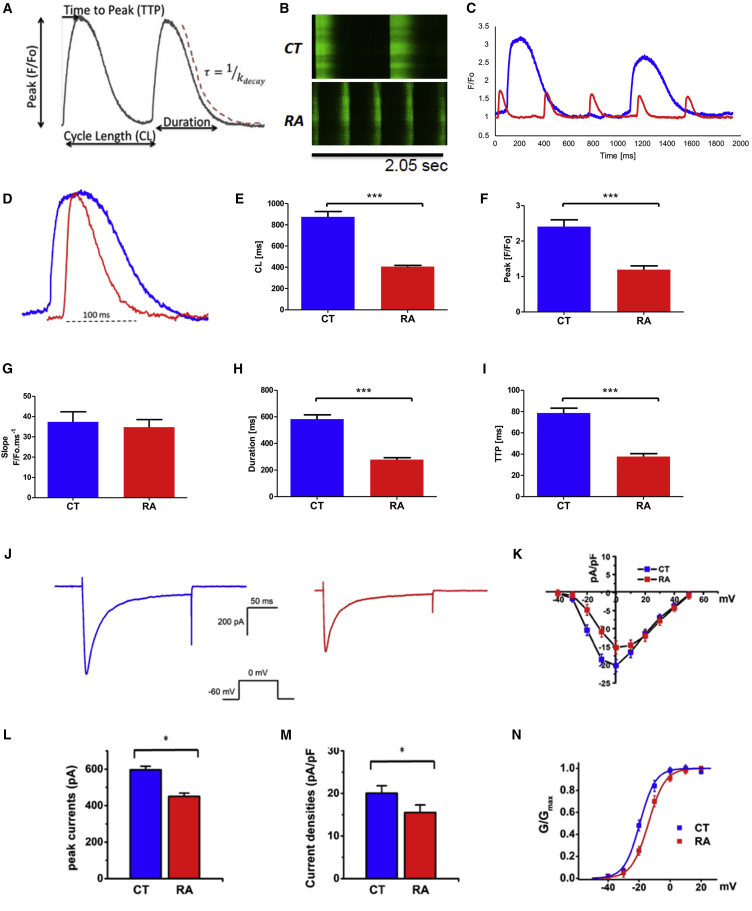
Human induced pluripotent stem cell (hiPSC)-derived atrial cardiomyocytes (CMs) hold great promise for elucidating underlying cellular mechanisms that cause atrial fibrillation (AF). In order to use atrial-like hiPSC-CMs for arrhythmia modeling, it is essential to better understand the molecular and electrophysiological phenotype of these cells. We performed comprehensive molecular, transcriptomic, and electrophysiologic analyses of retinoic acid (RA)-guided hiPSC atrial-like CMs and demonstrate that RA results in differential expression of genes involved in calcium ion homeostasis that directly interact with an RA receptor, chicken ovalbumin upstream promoter-transcription factor 2 (COUP-TFII). We report a mechanism by which RA generates an atrial-like electrophysiologic signature through the downstream regulation of calcium channel gene expression by COUP-TFII and modulation of calcium handling. Collectively, our results provide important insights into the underlying molecular mechanisms that regulate atrial-like hiPSC-CM electrophysiology and support the use of atrial-like CMs derived from hiPSCs to model AF.
Keywords: atrial fibrillation; cardiomyocytes; disease modeling; human induced pluripotent stem cells.
Copyright © 2018 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Devalla H.D., Schwach V., Ford J.W., Milnes J.T., El-Haou S., Jackson C., Gkatzis K., Elliott D.A., Chuva de Sousa Lopes S.M., Mummery C.L. Atrial-like cardiomyocytes from human pluripotent stem cells are a robust preclinical model for assessing atrial-selective pharmacology. EMBO Mol. Med. 2015;7:394–410. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
