

Hospitalized frail elderly patients - atrial fibrillation, anticoagulation and 12 months' outcomes
- PMID: 29731616
- PMCID: PMC5927348
- DOI: 10.2147/CIA.S159373
Hospitalized frail elderly patients - atrial fibrillation, anticoagulation and 12 months' outcomes
Abstract
Background and objective: Multiple chronic conditions and recurring acute illness are frequent among elderly people. One such condition is atrial fibrillation (AF), which increases the risk of stroke up to fivefold. The aim of this study was to investigate the prevalence of AF among hospitalized frail elderly patients, their use of anticoagulation and their 12-month outcomes.
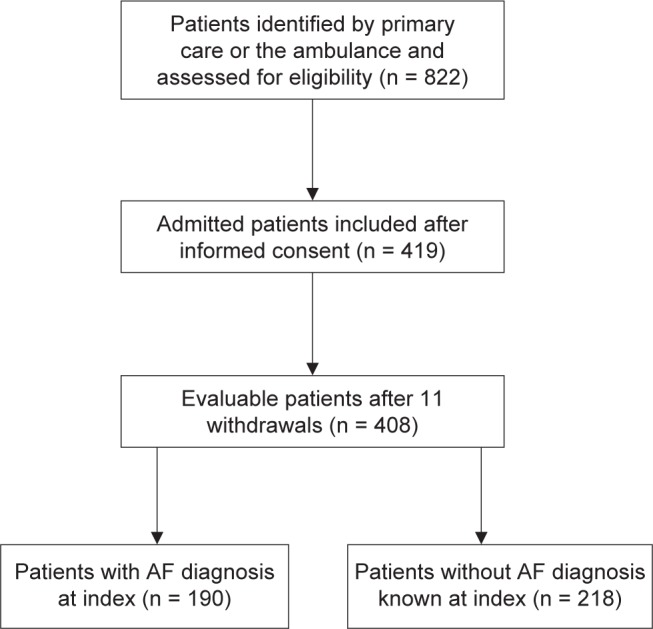
Patients and methods: This was a clinical observational study of acutely hospitalized frail patients over the age of 75 years. The CHA2DS2-VASc Score was used to evaluate ischemic stroke risk in patients with AF. Clinically relevant outcomes were the composite of ischemic stroke and/or bleeding within 12 months, which was considered as primary in the analysis, ischemic stroke/transient ischemic attack (TIA), mortality, bleeding and hospital care consumption. Student's t-test, Fisher's exact test, Mann-Whitney U test and a Cox proportional hazards model were used for the analyses.
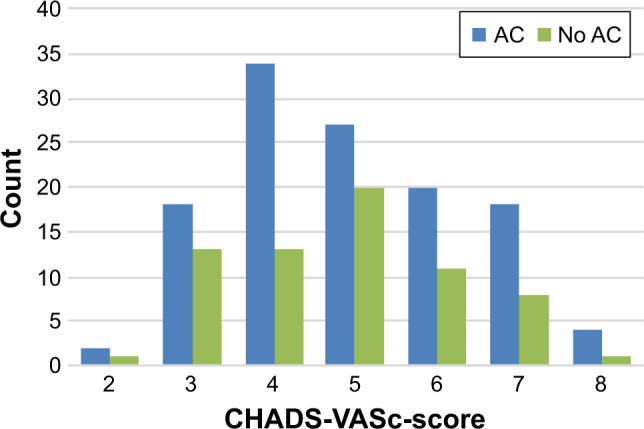
Results: The prevalence of AF was 47%, and 63% of them were prescribed an anticoagulant. AF patients without anticoagulation were older, more often females, more often in residential care, and they had worse Mini Nutritional Assessment and activities of daily living scores. Of the patients without anticoagulation, 56% had a documented contraindication. In univariate analysis, there were significantly more events among AF patients without anticoagulation regarding the composite outcome of ischemic stroke and/or bleeding (hazard ratio [HR] 3.65, 95% CI = 1.70-7.86; p < 0.001). When adjusting for potential confounders in Cox regression analysis, the difference remained significant (HR 4.54, 95% CI = 1.83-11.25; p = 0.001).
Conclusion: The prevalence of AF in a hospitalized frail elderly population was 47%. Of these, 63% were prescribed anticoagulation therapy. Almost half of the patients without stroke prophylaxis had no documented contraindication. At 1 year, there were significantly more events in terms of ischemic stroke and/or bleeding among AF patients without anticoagulation therapy than among those with.
Keywords: anticoagulants; atrial fibrillation; frail elderly; outcomes; patient safety.
Conflict of interest statement
Disclosure Dr Björn W Karlson is an employee of AstraZeneca. The other authors report no conflicts of interest in this work.
Figures
Similar articles
-
The HAS-BLED score has better prediction accuracy for major bleeding than CHADS2 or CHA2DS2-VASc scores in anticoagulated patients with atrial fibrillation.J Am Coll Cardiol. 2013 Dec 10;62(23):2199-204. doi: 10.1016/j.jacc.2013.08.1623. Epub 2013 Sep 18. J Am Coll Cardiol. 2013. PMID: 24055744
-
The Effect of Bleeding Risk and Frailty Status on Anticoagulation Patterns in Octogenarians With Atrial Fibrillation: The FRAIL-AF Study.Can J Cardiol. 2016 Feb;32(2):169-76. doi: 10.1016/j.cjca.2015.05.012. Epub 2015 May 27. Can J Cardiol. 2016. PMID: 26277091
-
Practice Patterns and Outcomes Associated With Use of Anticoagulation Among Patients With Atrial Fibrillation During Sepsis.JAMA Cardiol. 2016 Sep 1;1(6):682-90. doi: 10.1001/jamacardio.2016.2181. JAMA Cardiol. 2016. PMID: 27487456 Free PMC article.
-
Outcome of novel oral anticoagulant versus warfarin in frail elderly patients with atrial fibrillation: a systematic review and meta-analysis of retrospective studies.Acta Clin Belg. 2023 Oct;78(5):367-377. doi: 10.1080/17843286.2023.2179908. Epub 2023 Feb 22. Acta Clin Belg. 2023. PMID: 36814097
-
Reasons for undertreatment with oral anticoagulants in frail geriatric outpatients with atrial fibrillation: a prospective, descriptive study.Drugs Aging. 2010 Jan 1;27(1):39-50. doi: 10.2165/11319540-000000000-00000. Drugs Aging. 2010. PMID: 20030431 Review.
Cited by
-
Relationship between Pharmacological Treatment Strategy and Cognitive Function in Geriatric Patients with Atrial Fibrillation.J Clin Med. 2023 Dec 16;12(24):7724. doi: 10.3390/jcm12247724. J Clin Med. 2023. PMID: 38137793 Free PMC article.
-
The 2020 CCS atrial fibrillation guidelines for pharmacists: Top 10 takeaways.Can Pharm J (Ott). 2021 Nov 17;155(2):107-118. doi: 10.1177/17151635211058160. eCollection 2022 Mar-Apr. Can Pharm J (Ott). 2021. PMID: 35300017 Free PMC article. No abstract available.
-
[Prevalence, incidence and predictive factors of atrial fibrillation in geriatric patients-A prospective observational study].Z Gerontol Geriatr. 2024 Mar;57(2):120-125. doi: 10.1007/s00391-023-02177-0. Epub 2023 Apr 21. Z Gerontol Geriatr. 2024. PMID: 37084091 German.
-
Frailty and oral anticoagulant prescription in adults with atrial fibrillation: A systematic review.Aging Med (Milton). 2022 Jun 1;6(2):195-206. doi: 10.1002/agm2.12214. eCollection 2023 Jun. Aging Med (Milton). 2022. PMID: 37287671 Free PMC article. Review.
-
Comparison of Healthcare Resource Utilization and Costs between Rivaroxaban and Warfarin for Nonvalvular Atrial Fibrillation in a Skilled Nursing Facility Setting.Drugs Aging. 2020 Apr;37(4):281-289. doi: 10.1007/s40266-019-00737-x. Drugs Aging. 2020. PMID: 32147804
References
-
- World Health Organization (WHO) Fact sheet: Ageing and health 2015. [Accessed September 17, 2017]. Available from: http://www.who.int/mediacentre/factsheets/fs404/en/
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A: Biol Sci Med Sci. 2001;56:146–156. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
