

Minimally Invasive Bilateral Anterior Cingulotomy via Open Minicraniotomy Using a Novel Multiport Cisternoscope: A Cadaveric Demonstration
- PMID: 29733426
- PMCID: PMC6215753
- DOI: 10.1093/ons/opy083
Minimally Invasive Bilateral Anterior Cingulotomy via Open Minicraniotomy Using a Novel Multiport Cisternoscope: A Cadaveric Demonstration
Abstract
Background: Bilateral anterior cingulotomy has been used to treat chronic pain, obsessive compulsive disorder, and addictions. Lesioning of the target area is typically performed using bilateral stereotactic electrode placement and target ablation, which involves transparenchymal access through both hemispheres.
Objective: To evaluate an endoscopic direct-vision lesioning using a unilateral parasagittal minicraniotomy for minimally invasive bilateral anterior cingulotomy using a novel multiport endoscope through the anterior interhemispheric fissure.
Methods: A novel multiport magnetic resonance imaging (MRI)-compatible neuroendoscope prototype is used to demonstrate cadaveric cingulate lesioning through a lateral imaging port while simultaneously viewing the pericallosal arteries as landmarks through a tip imaging port. The lateral port enables extended lesioning of the gyrus while rotation of the endoscope about its axis provides access to homologous areas of both hemispheres.
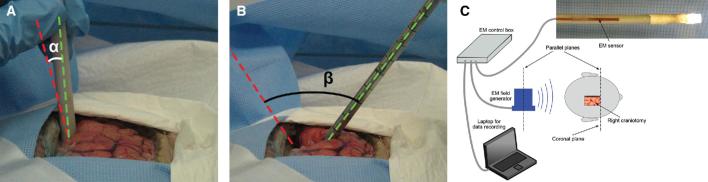
Results: Cadaver testing confirmed the capability to navigate the multiport neuroendoscope between the hemispheres using concurrent imaging from the tip and lateral ports. The lateral port enabled exploration of the gyrus, visualization of lesioning, and subsequent inspection of lesions. Tip-port imaging provided navigational cues and allowed the operator to ensure that the endoscope tip did not contact tissue. The multiport design required instrument rotation in the coronal plane of only 20° to lesion both gyri, while a standard endoscope necessitated a rotation of 54°.
Conclusion: Multiport MRI-compatible endoscopy can be effectively used in cisternal endoscopy, whereby a unilateral parasagittal minicraniotomy can be used for endoscopic interhemispheric bilateral anterior cingulotomy.
Figures







References
-
- Ramesh V, Balasubraminian C. Letter to the editor: obsessive-compulsive disorder and cingulotomy. J Neurosurg. 2013;119(2):526. - PubMed
-
- Banks GP, Mikell CB, Youngerman BEet al. Neuroanatomical characteristics associated with response to dorsal anterior cingulotomy for obsessive-compulsive disorder. JAMA Psychiatry. 2015;72(2):127-135. - PubMed
-
- Bourne SK, Sheth SA, Neal Jet al. Beneficial effect of subsequent lesion procedures after nonresponse to initial cingulotomy for severe, treatment-refractory obsessive-compulsive disorder. Neurosurgery. 2013;72(2):196-202. - PubMed
-
- De Ridder D, Leong SL, Manning P, Vanneste S, Glue P. Anterior cingulate implant for obsessive-compulsive disorder. World Neurosurg. 2017;97:754.e7-754.e16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
