

Pharmacokinetics, Pharmacodynamics, and Tolerability of Concomitant Multiple Dose Administration of Verinurad (RDEA3170) and Allopurinol in Adult Male Subjects With Gout
- PMID: 29733447
- PMCID: PMC6099444
- DOI: 10.1002/jcph.1119
Pharmacokinetics, Pharmacodynamics, and Tolerability of Concomitant Multiple Dose Administration of Verinurad (RDEA3170) and Allopurinol in Adult Male Subjects With Gout
Abstract
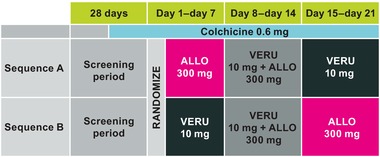
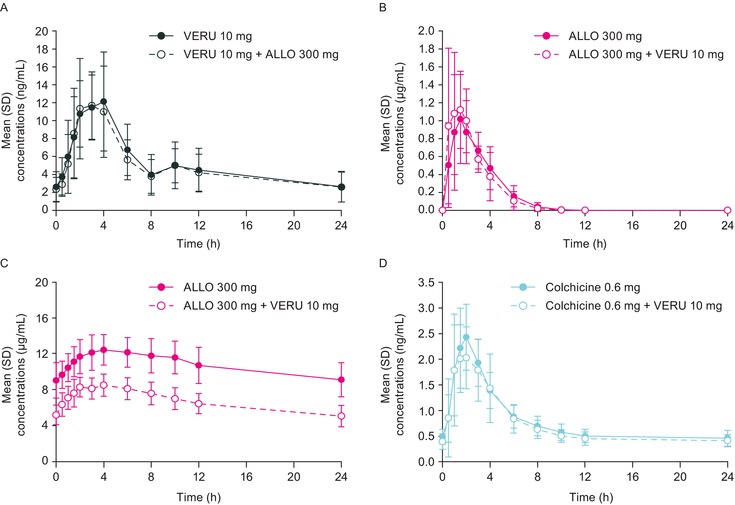
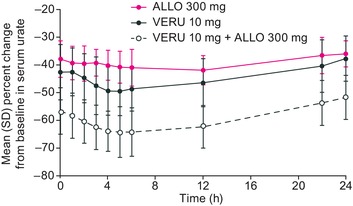
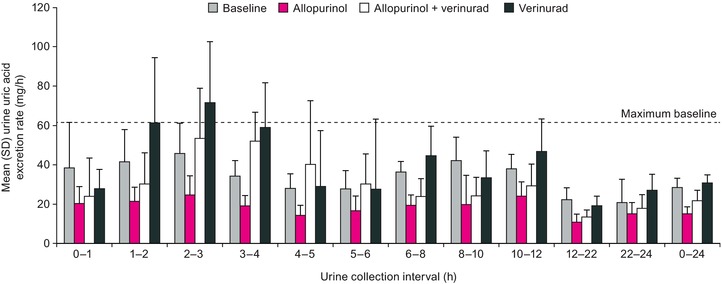
Verinurad (RDEA3170) is a selective uric acid reabsorption inhibitor in clinical development for treatment of hyperuricemia and gout. This phase 1b, multiple-dose, drug-drug interaction study evaluated the pharmacokinetics, pharmacodynamics, and tolerability of verinurad in combination with allopurinol. Adult males with gout were randomized to receive once-daily oral doses of allopurinol 300 mg or verinurad 10 mg alone for 7 days, allopurinol 300 mg + verinurad 10 mg on days 8 to 14, and the alternative single agent on days 15 to 21. Colchicine 0.6 mg was taken prophylactically for gout flares. Plasma/serum and urine samples were assayed for verinurad, allopurinol, oxypurinol (allopurinol active metabolite), colchicine (plasma only), and uric acid. Safety was assessed by adverse events (AEs) and laboratory tests. Verinurad plasma exposure was unaffected by allopurinol. Verinurad increased the maximum observed plasma concentration (Cmax ) for allopurinol by 33%; the area under the plasma concentration-time curve (AUC) was unaffected. Oxypurinol Cmax and AUC were reduced 32% and 38%, respectively, by verinurad. Colchicine plasma exposure was unaltered by verinurad. The maximum decrease in serum urate was greater with verinurad + allopurinol (65%) than with verinurad (51%) or allopurinol (43%) alone. Compared with the baseline rate, the maximum rate of uric acid excreted in urine was +56% with verinurad, -46% with allopurinol, and unchanged with verinurad + allopurinol. No serious AEs, discontinuations due to AEs, or clinically significant laboratory abnormalities were noted. Despite decreased systemic exposure of allopurinol and oxypurinol in the presence of verinurad, the combination resulted in greater serum urate reduction compared with either drug alone and was well tolerated at the studied doses.
Keywords: Pharmacokinetics; combination therapy; gout; pharmacodynamics; serum uric acid; tolerability.
© 2018, The Authors. The Journal of Clinical Pharmacology published by Wiley Periodicals, Inc. on behalf of American College of Clinical Pharmacology.
Figures
References
-
- Rees F, Hui M, Doherty M. Optimizing current treatment of gout. Nat Rev Rheumatol. 2014;10:271–283. - PubMed
-
- Doherty M, Jansen TL, Nuki G, et al. Gout: why is this curable disease so seldom cured? Ann Rheum Dis. 2012;71:1765–1770. - PubMed
-
- Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence‐based recommendations for the management of gout. Ann Rheum Dis. 2017;76:29–42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
