

Orthostatic Hypotension and Risk of Clinical and Subclinical Cardiovascular Disease in Middle-Aged Adults
- PMID: 29735525
- PMCID: PMC6015335
- DOI: 10.1161/JAHA.118.008884
Orthostatic Hypotension and Risk of Clinical and Subclinical Cardiovascular Disease in Middle-Aged Adults
Abstract
Background: Although orthostatic hypotension (OH) is a well-recognized manifestation of neuropathy and hypovolemia, its contribution to cardiovascular disease (CVD) risk is controversial.
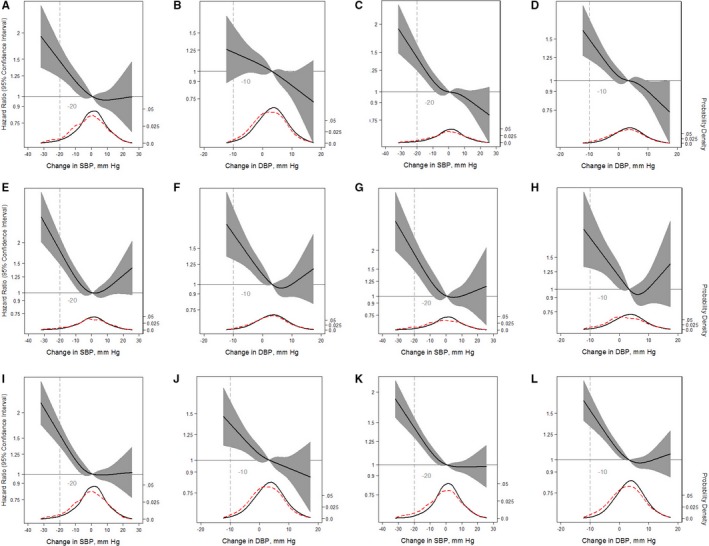
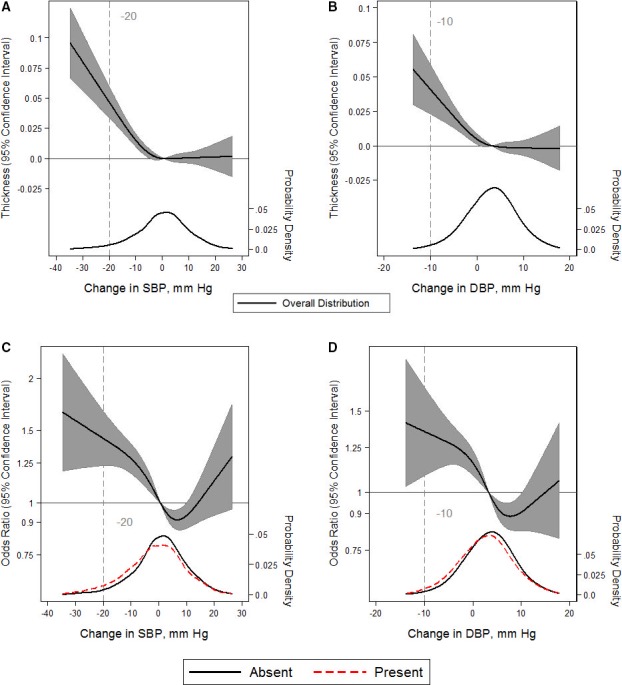
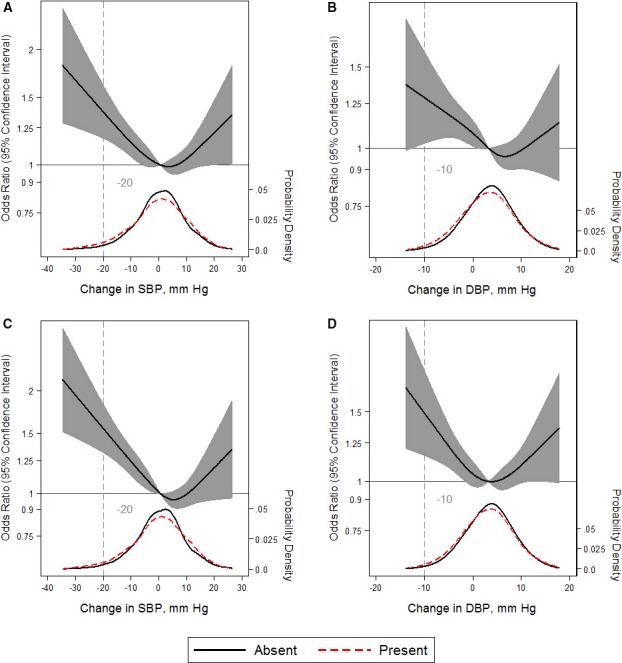
Methods and results: Participants with OH, defined as a decrease in blood pressure (systolic ≥20 mm Hg or diastolic ≥10 mm Hg) from the supine to standing position, were identified during the first visit of the ARIC (Atherosclerosis Risk in Communities) Study (1987-1989) within 2 minutes of standing. All participants were followed up for the development of myocardial infarction, heart failure, stroke, fatal coronary heart disease (CHD), any CHD (combination of silent, nonfatal, and fatal CHD or cardiac procedures), and all-cause mortality. Participants were assessed for carotid intimal thickness and plaque during the first visit. Detectable high-sensitivity troponin T (≥5 ng/L) and elevated NT-proBNP (N-terminal pro-B-type natriuretic peptide; ≥100 pg/mL) were determined in blood collected during the second visit (1990-1992). All associations were adjusted for known CVD risk factors. In 9139 participants (57% women; 23% black; mean age, 54±5.7 years), 3% had OH. During follow-up (median, 26 years), OH was associated with myocardial infarction (hazard ratio [HR], 1.88; 95% confidence interval [CI], 1.44-2.46), congestive heart failure (HR, 1.65; 95% CI, 1.34-2.04), stroke (HR, 1.83; 95% CI, 1.35-2.48), fatal CHD (HR, 2.77; 95% CI, 1.93-3.98), any CHD (HR, 2.00; 95% CI, 1.64-2.44), and all-cause mortality (HR, 1.68; 95% CI, 1.45-1.95). OH was also associated with carotid intimal thickness (β, 0.05 mm; 95% CI, 0.04-0.07 mm), carotid plaque (odds ratio, 1.51; 95% CI, 1.18-1.93), detectable high-sensitivity troponin T (odds ratio, 1.49; 95% CI, 1.16-1.93), and elevated NT-proBNP (odds ratio, 1.92; 95% CI, 1.48-2.49).
Conclusions: OH identified in community-dwelling middle-aged adults was associated with future CVD events and subclinical CVD. Further research is necessary to establish a causal role for OH in the pathogenesis of CVD.
Keywords: NT‐proBNP; cardiovascular disease; heart failure; high‐sensitivity troponin; mortality; orthostatic hypotension; stroke.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Press Y, Punchik B, Freud T. Orthostatic hypotension and drug therapy in patients at an outpatient comprehensive geriatric assessment unit. J Hypertens. 2016;34:351–358. - PubMed
-
- Wu J‐S, Yang Y‐C, Lu F‐H, Wu C‐H, Chang C‐J. Population‐based study on the prevalence and correlates of orthostatic hypotension/hypertension and orthostatic dizziness. Hypertens Res. 2008;31:897–904. - PubMed
-
- Shin C, Abbott RD, Lee H, Kim J, Kimm K. Prevalence and correlates of orthostatic hypotension in middle‐aged men and women in Korea: the Korean Health and Genome Study. J Hum Hypertens. 2004;18:717–723. - PubMed
-
- Juraschek SP, Daya N, Rawlings AM, Appel LJ, Miller ER, Windham BG, Griswold ME, Heiss G, Selvin E. Association of history of dizziness and long‐term adverse outcomes with early vs later orthostatic hypotension assessment times in middle‐aged adults. JAMA Intern Med. 2017;177:1316–1323. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201700005I/NHLBI NIH HHS/National Heart, Lung, and Blood Institute/United States
- HHSN268201700001I/NHLBI NIH HHS/National Heart, Lung, and Blood Institute/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- HHSN268201700002I/NHLBI NIH HHS/National Heart, Lung, and Blood Institute/United States
- HHSN268201700003I/NHLBI NIH HHS/National Heart, Lung, and Blood Institute/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
