

ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade
- PMID: 29736026
- PMCID: PMC6076433
- DOI: 10.1038/s41591-018-0012-z
ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade
Abstract
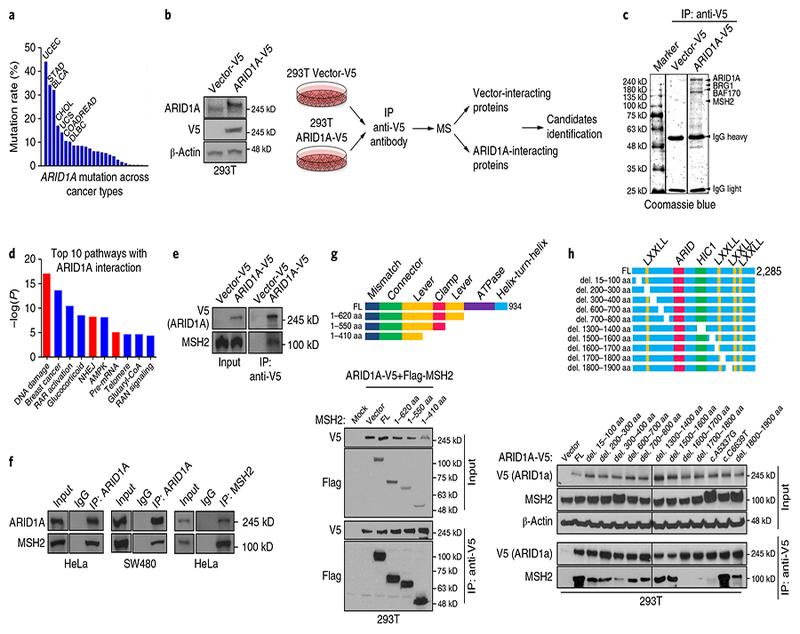
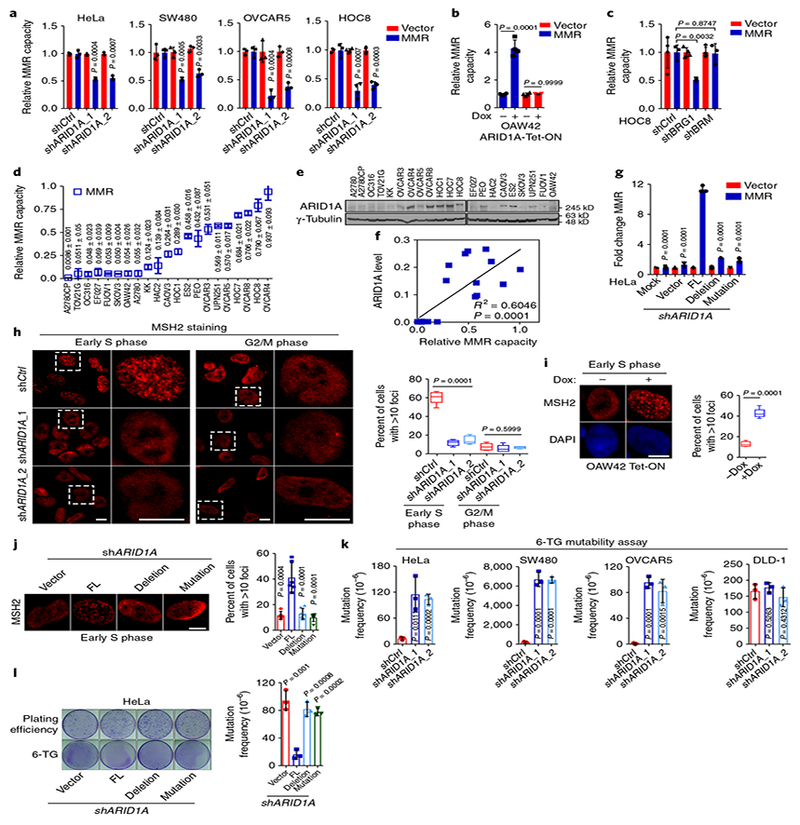
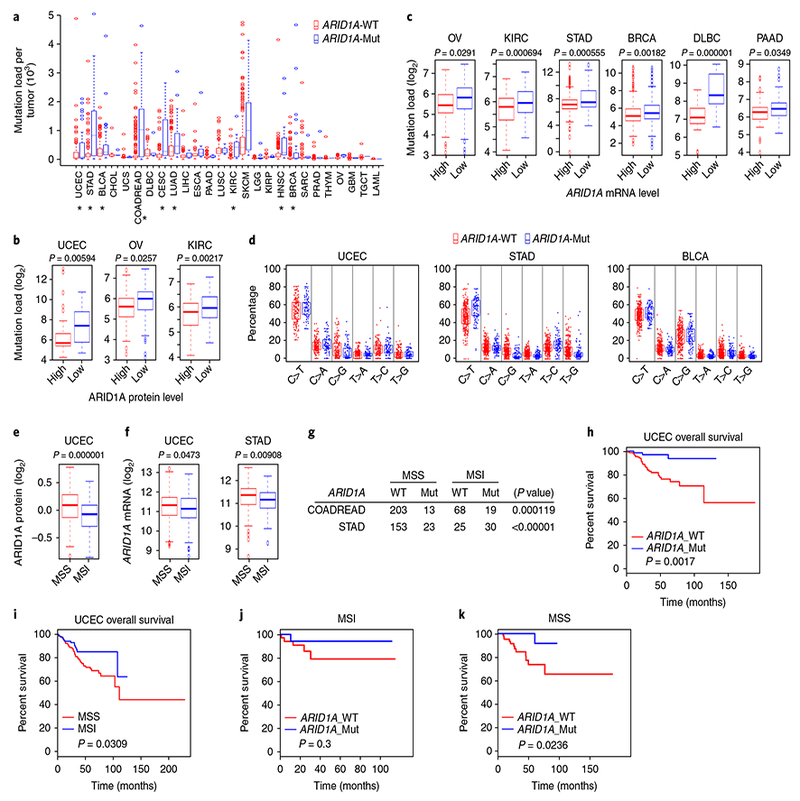
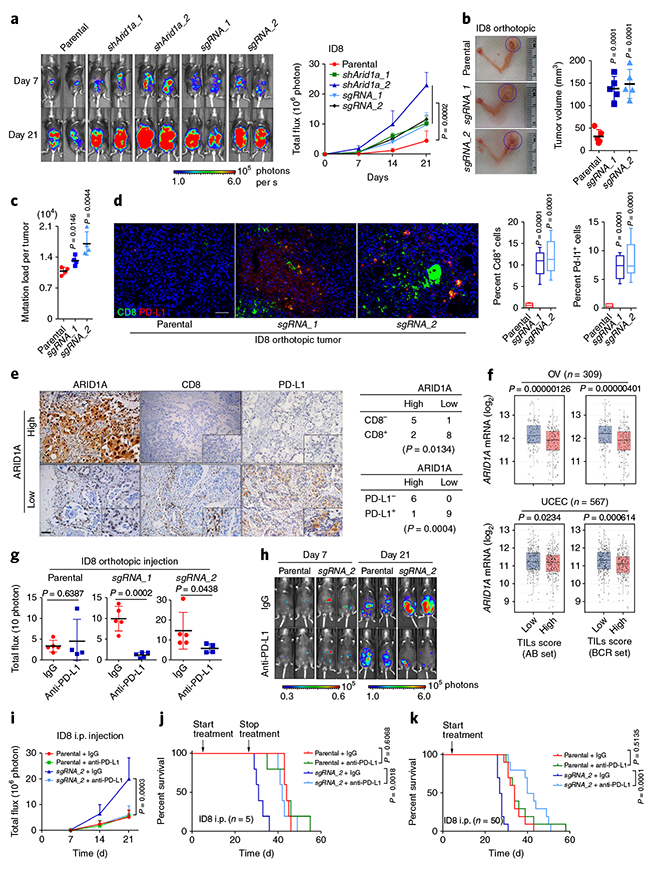
ARID1A (the AT-rich interaction domain 1A, also known as BAF250a) is one of the most commonly mutated genes in cancer1,2. The majority of ARID1A mutations are inactivating mutations and lead to loss of ARID1A expression 3 , which makes ARID1A a poor therapeutic target. Therefore, it is of clinical importance to identify molecular consequences of ARID1A deficiency that create therapeutic vulnerabilities in ARID1A-mutant tumors. In a proteomic screen, we found that ARID1A interacts with mismatch repair (MMR) protein MSH2. ARID1A recruited MSH2 to chromatin during DNA replication and promoted MMR. Conversely, ARID1A inactivation compromised MMR and increased mutagenesis. ARID1A deficiency correlated with microsatellite instability genomic signature and a predominant C>T mutation pattern and increased mutation load across multiple human cancer types. Tumors formed by an ARID1A-deficient ovarian cancer cell line in syngeneic mice displayed increased mutation load, elevated numbers of tumor-infiltrating lymphocytes, and PD-L1 expression. Notably, treatment with anti-PD-L1 antibody reduced tumor burden and prolonged survival of mice bearing ARID1A-deficient but not ARID1A-wild-type ovarian tumors. Together, these results suggest ARID1A deficiency contributes to impaired MMR and mutator phenotype in cancer, and may cooperate with immune checkpoint blockade therapy.
Conflict of interest statement
Competing interests
G.B.M. has received sponsored research support from Abbvie, AstraZeneca, Critical Outcomes Technology, Horizon Diagnostics, Illumina, Immunomet, Ionis, Karus Therapeutics, Nanostring, Pfizer, Takeda/Millennium Pharmaceuticals, and Tesaro; has ownership interest in Catena Pharmaceuticals, PTV Ventures, and Spindle Top Ventures; and is a consultant/advisory board member of AstraZeneca, Catena Pharmaceuticals, Critical Outcome Technologies, ImmunoMET, Ionis, Medimmune, Nuevolution, Pfizer, Precision Medicine, Signalchem Lifesciences, Symphogen, Takeda/Millennium Pharmaceuticals, and Tarveda. G.P. has received sponsored research support from Pifzer. No potential conflicts of interest were disclosed by the other authors.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
