

Gastric Cancer Maximum Tumour Diameter Reduction Rate at CT Examination as a Radiological Index for Predicting Histopathological Regression after Neoadjuvant Treatment: A Multicentre GIRCG Study
- PMID: 29736166
- PMCID: PMC5875045
- DOI: 10.1155/2018/1794524
Gastric Cancer Maximum Tumour Diameter Reduction Rate at CT Examination as a Radiological Index for Predicting Histopathological Regression after Neoadjuvant Treatment: A Multicentre GIRCG Study
Abstract
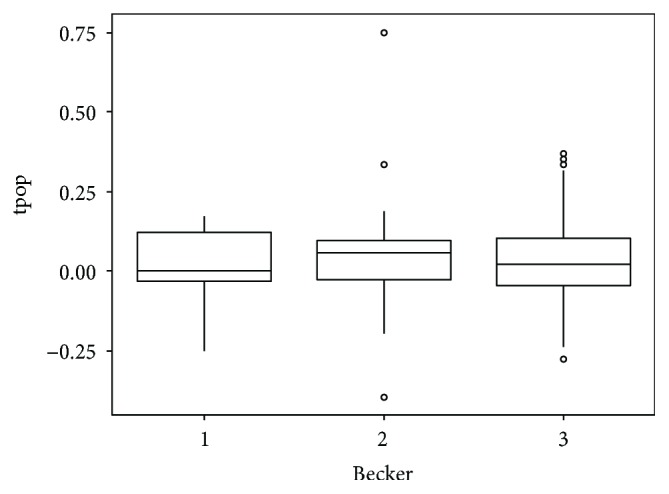
Aim: To investigate the role of maximum tumour diameter (D-max) reduction rate at CT examination in predicting histopathological tumour regression grade (TRG according to the Becker grade), after neoadjuvant chemotherapy (NAC), in patients with resectable advanced gastric cancer (AGC).
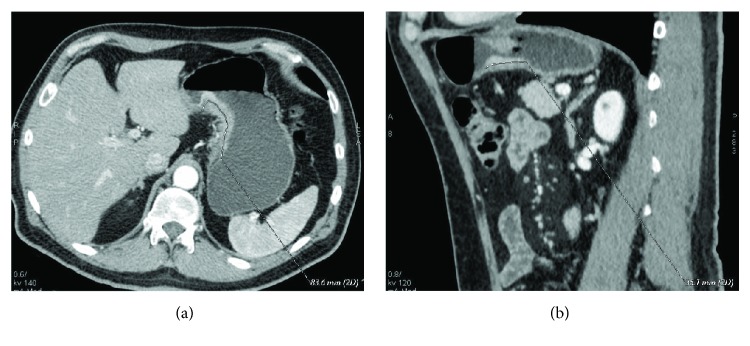
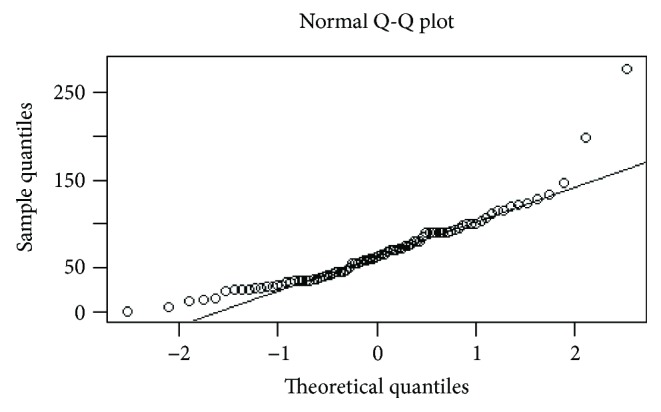
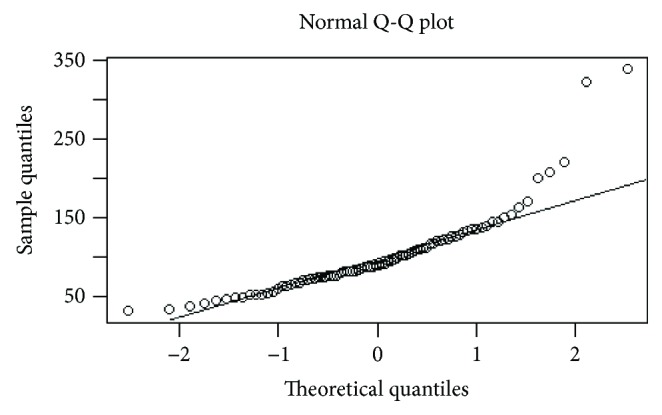
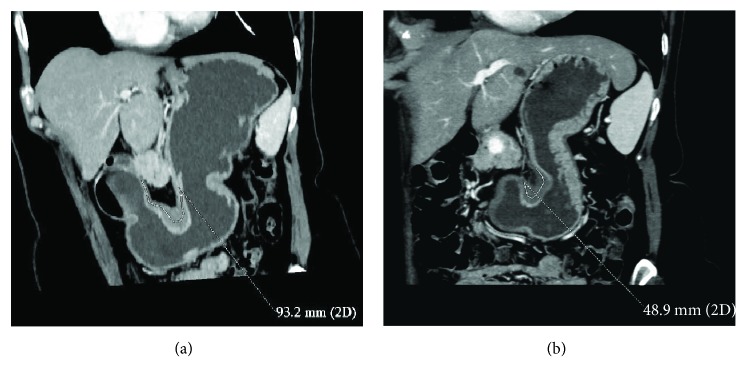
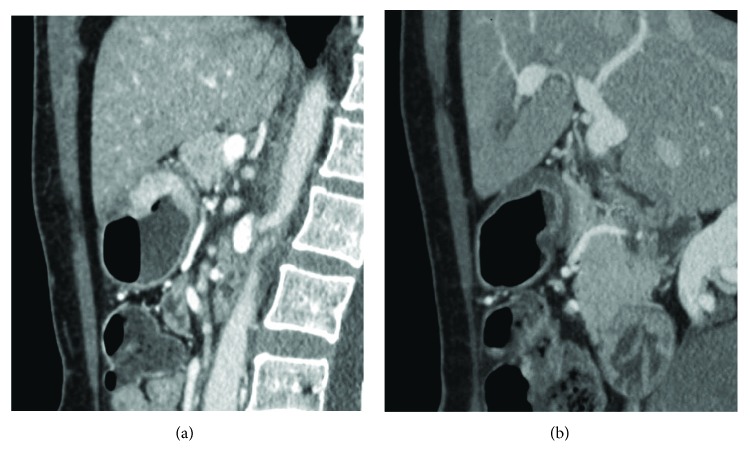
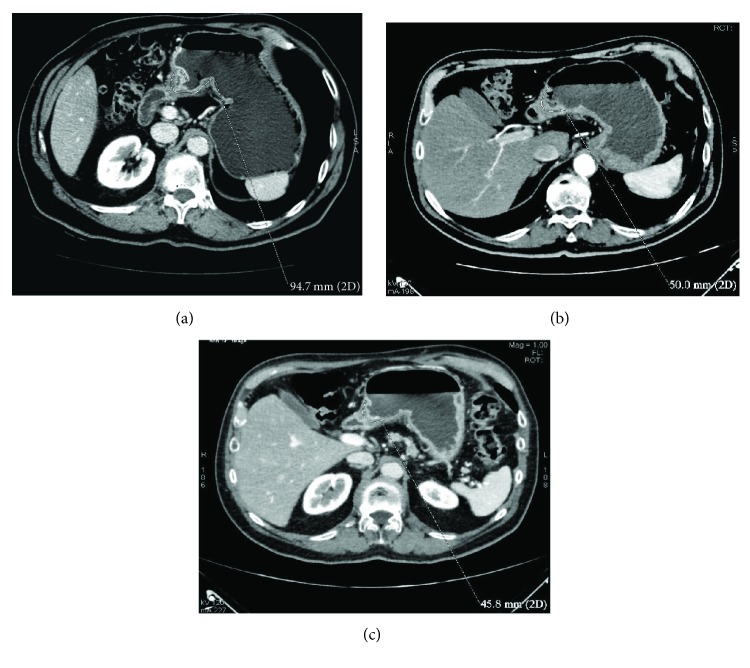
Materials and methods: Eighty-six patients (53 M, mean age 62.1 years) with resectable AGC (≥T3 or N+), treated with NAC and radical surgery, were enrolled from 5 centres of the Italian Research Group for Gastric Cancer (GIRCG). Staging and restaging CT and histological results were retrospectively reviewed. CT examinations were contrast enhanced, and the stomach was previously distended. The D-max was measured using 2D software and compared with Becker TRG. Statistical data were obtained using "R" software.
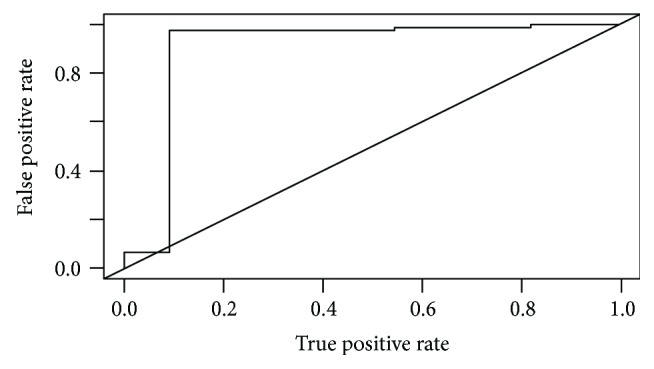
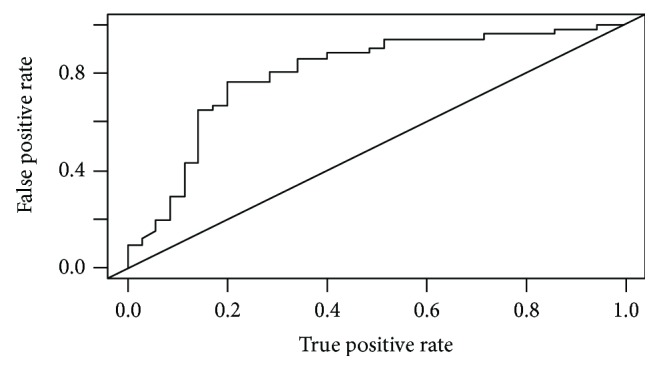
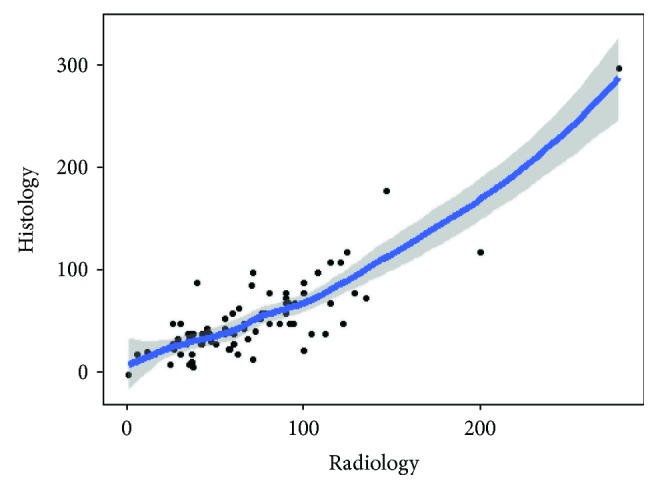
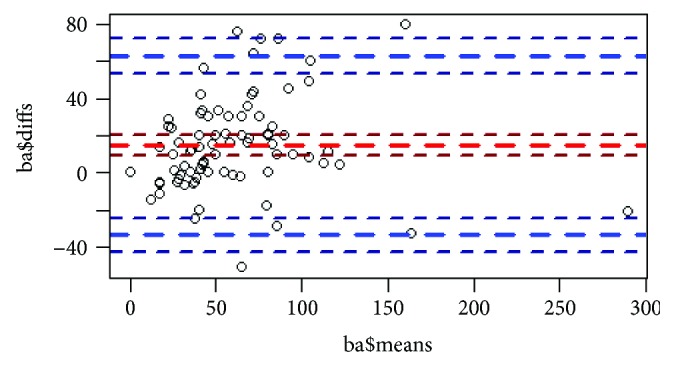
Results: The interobserver agreement was good/very good. Becker TRG was predicted by CT with a sensitivity and specificity, respectively, of 97.3% and 90.9% for Becker 1 (D-max reduction rate > 65.1%), 76.4% and 80% for Becker 3 (D-max reduction rate < 29.9%), and 70.8% and 83.9% for Becker 2. Correlation between radiological and histological D-max measurements was strongly confirmed by the correlation index (c.i.= 0.829).
Conclusions: D-max reduction rate in AGC patients may be helpful as a simple and reproducible radiological index in predicting TRG after NAC.
Figures

References
-
- Amin M. B., Edge S., Greene F., et al. AJCC Cancer Staging Manual. 8th. New York, NY, USA: Springer; 2017.
LinkOut - more resources
Full Text Sources
Other Literature Sources
