

The Impact of ESR1 Mutations on the Treatment of Metastatic Breast Cancer
- PMID: 29736566
- PMCID: PMC9680193
- DOI: 10.1007/s12672-017-0306-5
The Impact of ESR1 Mutations on the Treatment of Metastatic Breast Cancer
Abstract
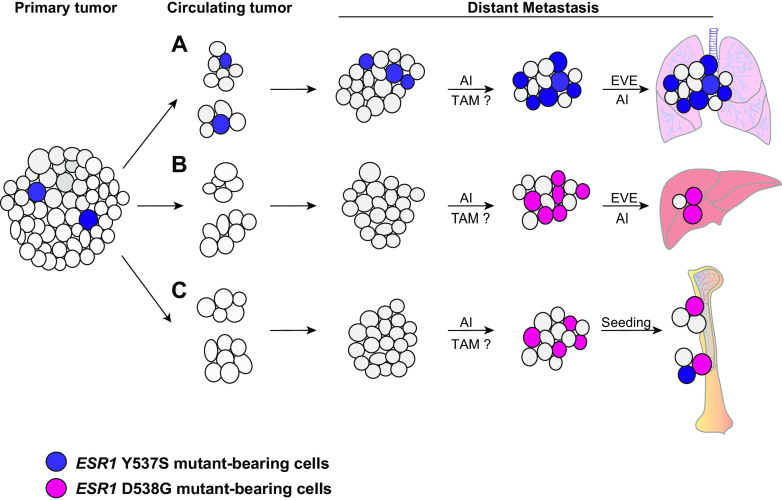
After nearly 20 years of research, it is now established that mutations within the estrogen receptor (ER) gene, ESR1, frequently occur in metastatic breast cancer and influence response to hormone therapy. Though early studies presented differing results, sensitive sequencing techniques now show that ESR1 mutations occur at a frequency between 20 and 40% depending on the assay method. Recent studies have focused on several "hot spot mutations," a cluster of mutations found in the hormone-binding domain of the ESR1 gene. Throughout the course of treatment, tumor evolution can occur, and ESR1 mutations emerge and become enriched in the metastatic setting. Sensitive techniques to continually monitor mutant burden in vivo are needed to effectively treat patients with mutant ESR1. The full impact of these mutations on tumor response to different therapies remains to be determined. However, recent studies indicate that mutant-bearing tumors may be less responsive to specific hormonal therapies, and suggest that aromatase inhibitor (AI) therapy may select for the emergence of ESR1 mutations. Additionally, different mutations may respond discretely to targeted therapies. The need for more preclinical mechanistic studies on ESR1 mutations and the development of better agents to target these mutations are urgently needed. In the future, sequential monitoring of ESR1 mutational status will likely direct personalized therapeutic regimens appropriate to each tumor's unique mutational landscape.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Hull DF, 3rd, Clark GM, Osborne CK, Chamness GC, Knight WA, 3rd, McGuire WL. Multiple estrogen receptor assays in human breast cancer. Cancer Res. 1983;43(1):413–416. - PubMed
-
- Gutierrez MC, Detre S, Johnston S, Mohsin SK, Shou J, Allred DC, Schiff R, Osborne CK, Dowsett M. Molecular changes in tamoxifen-resistant breast cancer: relationship between estrogen receptor, HER-2, and p38 mitogen-activated protein kinase. J Clin Oncol. 2005;23(11):2469–2476. doi: 10.1200/JCO.2005.01.172. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
