

Review
doi: 10.1007/s12350-018-1293-9.
Epub 2018 May 7.
Cardiac MRI for the evaluation of oncologic cardiotoxicity
Affiliations
- PMID: 29736616
- PMCID: PMC6222005
- DOI: 10.1007/s12350-018-1293-9
Item in Clipboard
Review
Cardiac MRI for the evaluation of oncologic cardiotoxicity
J Nucl Cardiol.
2018 Dec.
Abstract
Cancer therapeutics-related cardiac dysfunction (CTRCD) is a well-established adverse effect resulting from a number of cancer therapeutics. Newer immunotherapy has been associated with cardiomyopathy and myocarditis making comprehensive imaging useful for early recognition. Cardiac MRI (CMR) offers a comprehensive evaluation to detect CTRCD. Established guidelines for monitoring left ventricular ejection fraction for potential cardiotoxicity have recently incorporated CMR. We will review the utility of CMR in contemporary evaluation for potential oncologic cardiotoxicity.
Keywords: Cardiac MRI; cardiac toxicity; cardio-oncology.
Figures
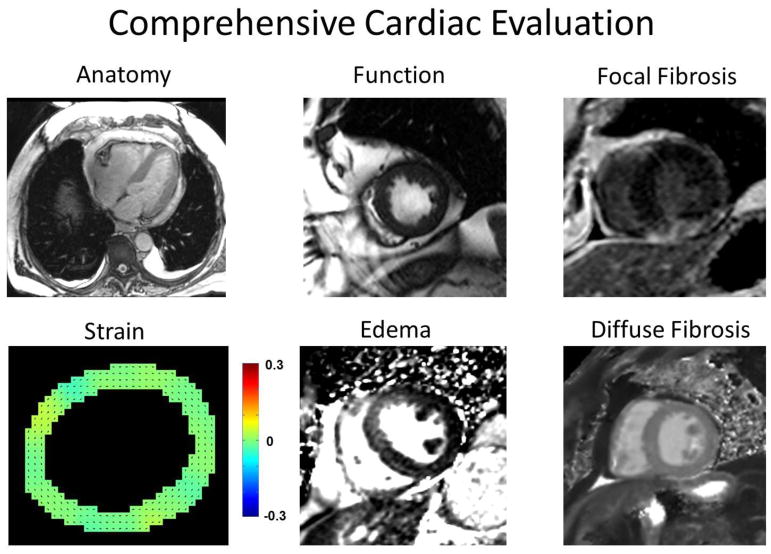
Demonstration of the comprehensive myocardial evaluation offered by CMR.
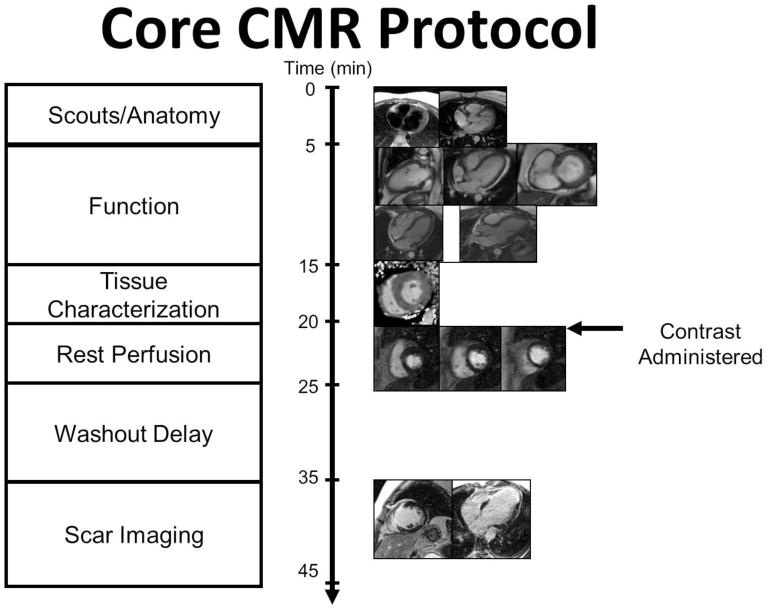
Basic CMR imaging protocol.
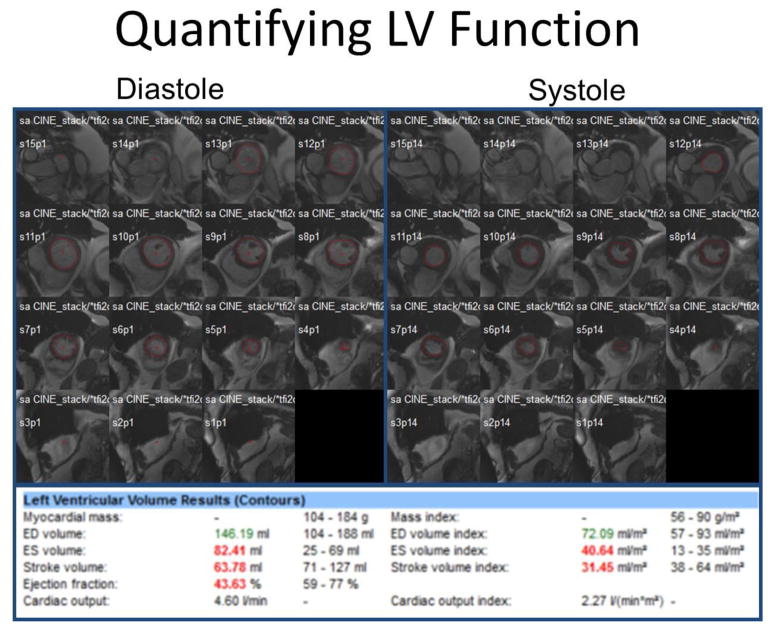
For LV chamber quantification, endocardial (red) contours are delineated at end-diastole (left) and end-systole (right) in a stack of short axis slices that cover the entire left ventricle. Computer-aided analysis packages are used to calculate LV parameters as shown. This patient has a decrease in EF and increase in end-systolic volume which can be seen in CTRCD.
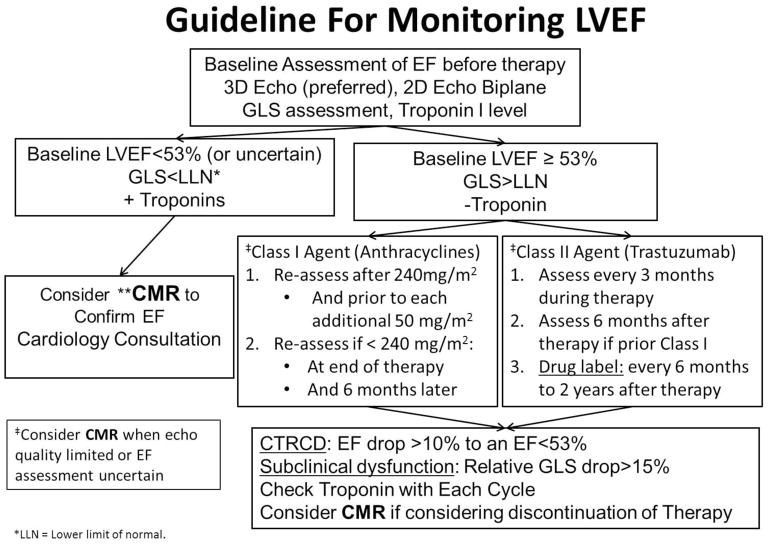
Guideline for monitoring LVEF for Class I and Class II agents adapted from Plana JC et. al. J Am Soc Echocardiogr 2014;27:911–39. ** CMR should be considered in high risk patients for cardiotoxicity when echo quality is limited or EF is uncertain. A non-contrast abbreviated protocol for EF assessment can be used at baseline and follow-up at intervals directed above. CMR with gadolinium can be used when there are concerns for myocarditis or scar imaging is necessary.
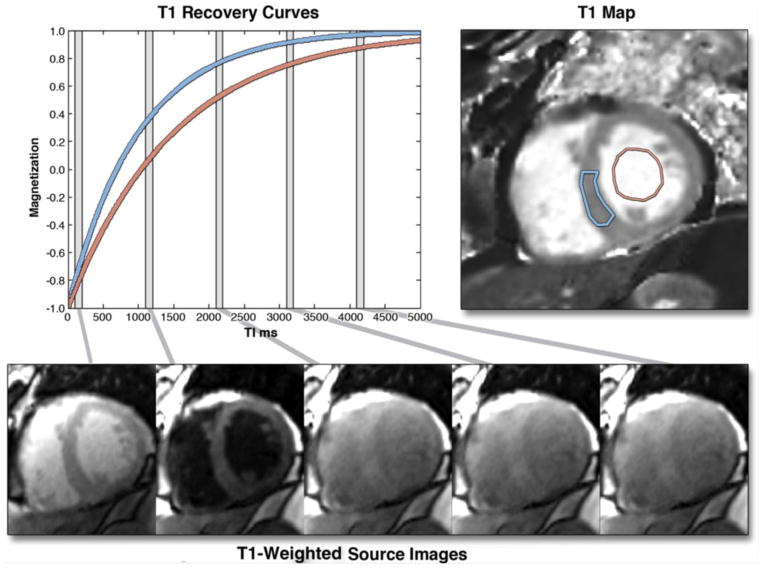
The graph on the left shows 2 inversion recovery curves for a septal region of interest (blue) and the blood pool, generated from images, shown in the bottom row, taken at different times after an inversion pulse at time t = 0. Similar inversion recovery curves can be generated for each pixel location if the images are all acquired during a breath-hold and for the same cardiac phase. The T1 for each pixel location can be used to generate a T1 map, as shown in the top-right image. T1 maps represent arguably the most succinct and informative summary of the spatial and temporal changes during an inversion recovery. Borrowed with permission from Taylor et al. JACC: Cardiovascular Imaging. 2016.
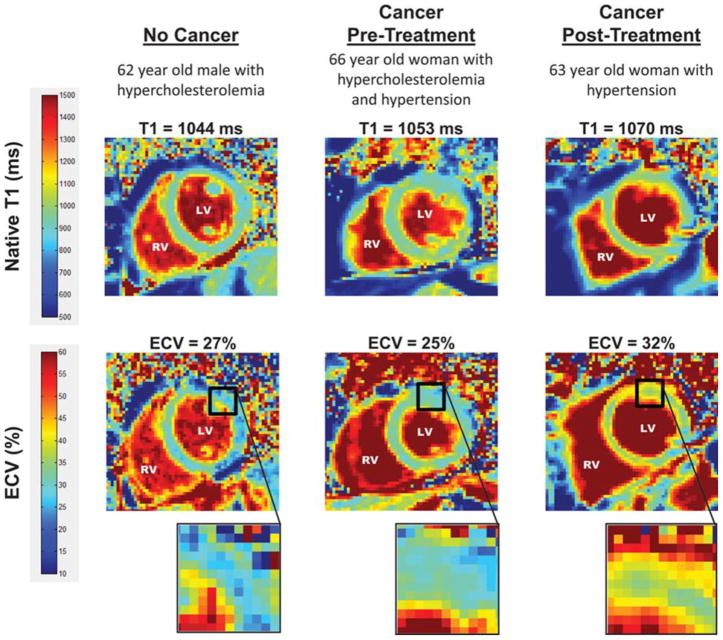
T1 and ECV map images. Representative left ventricular (LV) short-axis native T1 (top row) and extracellular volume (ECV, bottom row) maps are shown in similarly-aged participants. The LV and right ventricular (RV) blood pool cavities are noted. On each image, the color of pixels in the images (color scales on left) identifies the native T1 (milliseconds) and ECV (%). Insets on the ECV maps demonstrate the change in color intensity within the anterolateral wall of each ventricle. As shown, ECV is elevated in the cancer survivor previously treated with anthracycline-based chemotherapy. Borrowed with permission from Jordan et al. Circulation Imaging. 2016.
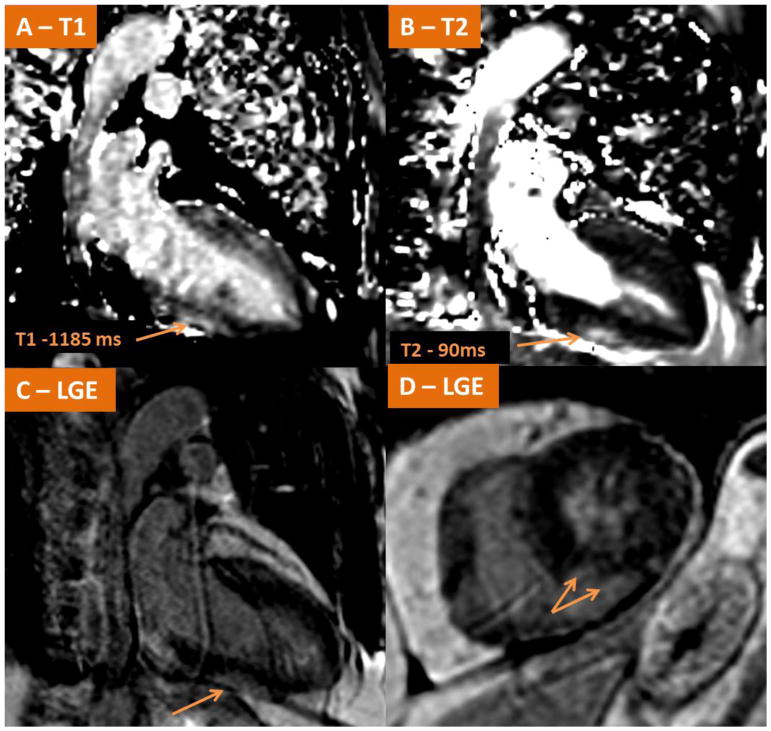
Demonstrates CMR findings in a case of acute fulminant myocarditis in a patient with metastatic melanoma shortly after receiving his first cycle of Ipilimumab/Nivolumab. (A–B) Native T1-mapping and T2 mapping respectively demonstrating elevated signals along the inferior wall consistent with myocardial edema. LGE imaging (C–D) demonstrate LGE present in the subepicardial mid inferior wall consistent with acute myocarditis.
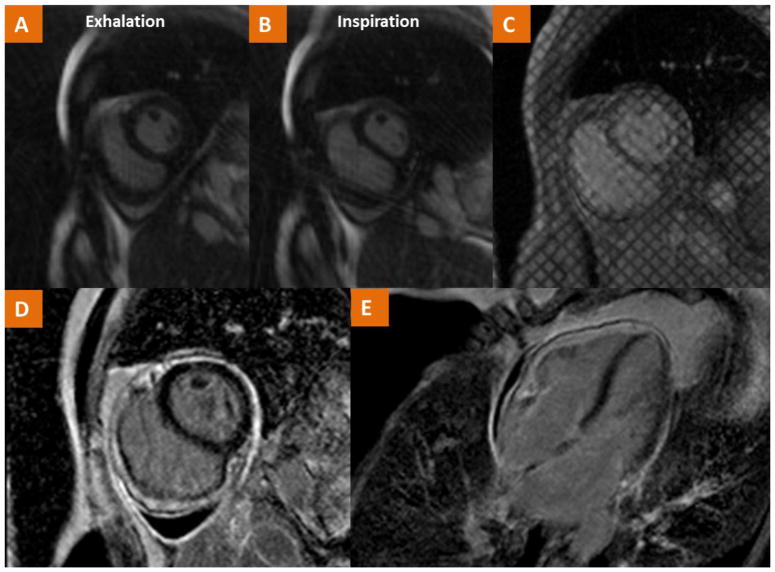
CMR findings in a case of a 54 year old female with history of Hodgkin’s Lymphoma treated with radiation at ages 20, 24, 27 and now with recurrent pericardial effusion and dyspnea. (A–B) Real-time cine imaging demonstrates flattening of the septum during inspiration consistent with ventricular interdependence as well as a small pericardial effusion. (C) Tagged cine gradient imaging used to detect fibrotic adhesion of pericardial layers. (D–E) LGE imaging demonstrates pericardial LGE consistent with pericardial inflammation. The consolidation of these findings is consistent with the diagnosis of pericardial constriction.
Similar articles
-
Serial Cardiovascular Magnetic Resonance Strain Measurements to Identify Cardiotoxicity in Breast Cancer: Comparison With Echocardiography.JACC Cardiovasc Imaging. 2021 May;14(5):962-974. doi: 10.1016/j.jcmg.2020.09.039. Epub 2020 Nov 25. JACC Cardiovasc Imaging. 2021. PMID: 33248962
-
Nuclear cardiology in the context of multimodality imaging to detect cardiac toxicity from cancer therapeutics: Established and emerging methods.J Nucl Cardiol. 2020 Aug;27(4):1210-1224. doi: 10.1007/s12350-019-01671-6. Epub 2019 Mar 13. J Nucl Cardiol. 2020. PMID: 30868378 Review.
-
Myocardial injury detected by T1 and T2 mapping on CMR predicts subsequent cancer therapy-related cardiac dysfunction in patients with breast cancer treated by epirubicin-based chemotherapy or left-sided RT.Eur Radiol. 2022 Mar;32(3):1853-1865. doi: 10.1007/s00330-021-08260-7. Epub 2021 Sep 18. Eur Radiol. 2022. PMID: 34536111 Free PMC article.
-
Improving reproducibility of left ventricular ejection fraction in pediatric oncology patients: less is more.Int J Cardiovasc Imaging. 2020 Oct;36(10):1887-1895. doi: 10.1007/s10554-020-01901-w. Epub 2020 Jun 2. Int J Cardiovasc Imaging. 2020. PMID: 32488453
-
Contemporary Role of Echocardiography for Clinical Decision Making in Patients During and After Cancer Therapy.JACC Cardiovasc Imaging. 2018 Aug;11(8):1122-1131. doi: 10.1016/j.jcmg.2018.03.025. JACC Cardiovasc Imaging. 2018. PMID: 30092969 Review.
Cited by
-
Novel Functional Radiomics for Prediction of Cardiac Positron Emission Tomography Avidity in Lung Cancer Radiotherapy.JCO Clin Cancer Inform. 2024 Mar;8:e2300241. doi: 10.1200/CCI.23.00241. JCO Clin Cancer Inform. 2024. PMID: 38452302 Free PMC article.
-
Cardiovascular Imaging in Cardio-Oncology: The Role of Echocardiography and Cardiac MRI in Modern Cardio-Oncology.Heart Fail Clin. 2022 Jul;18(3):455-478. doi: 10.1016/j.hfc.2022.02.007. Heart Fail Clin. 2022. PMID: 35718419 Free PMC article. Review.
-
Imaging of Cancer Immunotherapy: Current Approaches and Future Directions.Radiology. 2019 Jan;290(1):9-22. doi: 10.1148/radiol.2018181349. Epub 2018 Nov 20. Radiology. 2019. PMID: 30457485 Free PMC article. Review.
-
Assessment and Management of Cardiotoxicity in Hematologic Malignancies.Dis Markers. 2021 Feb 3;2021:6616265. doi: 10.1155/2021/6616265. eCollection 2021. Dis Markers. 2021. PMID: 33613788 Free PMC article. Review.
-
Emerging Challenges of Radiation-Associated Cardiovascular Dysfunction (RACVD) in Modern Radiation Oncology: Clinical Practice, Bench Investigation, and Multidisciplinary Care.Front Cardiovasc Med. 2020 Feb 21;7:16. doi: 10.3389/fcvm.2020.00016. eCollection 2020. Front Cardiovasc Med. 2020. PMID: 32154267 Free PMC article. Review.
References
-
- Tan C, Tasaka H, Yu KP, Murphy ML, Karnofsky DA. Daunomycin, an antitumor antibiotic, in the treatment of neoplastic disease. clinical evaluation with special reference to childhood leukemia. Cancer. 1967;20:333–53. - PubMed
-
- Alexander J, Dainiak N, Berger HJ, Goldman L, Johnstone D, Reduto L, et al. Serial assessment of doxorubicin cardiotoxicity with quantitative radionuclide angiocardiography. N Engl J Med. 1979;300:278–83. - PubMed
-
- Schwartz RG, McKenzie WB, Alexander J, Sager P, D’Souza A, Manatunga A, et al. Congestive heart failure and left ventricular dysfunction complicating doxorubicin therapy: Seven-year experience using serial radionuclide angiocardiography. The American Journal of Medicine. 1987;82:1109–18. - PubMed
-
- Seidman A, Hudis C, Pierri MK, Shak S, Paton V, Ashby M, et al. Cardiac dysfunction in the trastuzumab clinical trials experience. J Clin Oncol. 2002;20:1215–21. - PubMed
-
- Poust JC, Woolery JE, Green MR. Management of toxicities associated with high-dose interleukin-2 and biochemotherapy. Anticancer Drugs. 2013;24:1–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
