

A Novel Indirect Reduction Technique in Ankle Syndesmotic Injuries: A Cadaveric Study
- PMID: 29738403
- PMCID: PMC6008185
- DOI: 10.1097/BOT.0000000000001169
A Novel Indirect Reduction Technique in Ankle Syndesmotic Injuries: A Cadaveric Study
Abstract
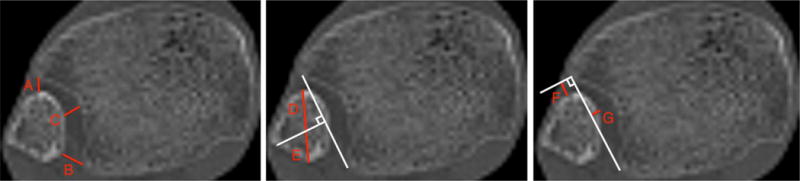
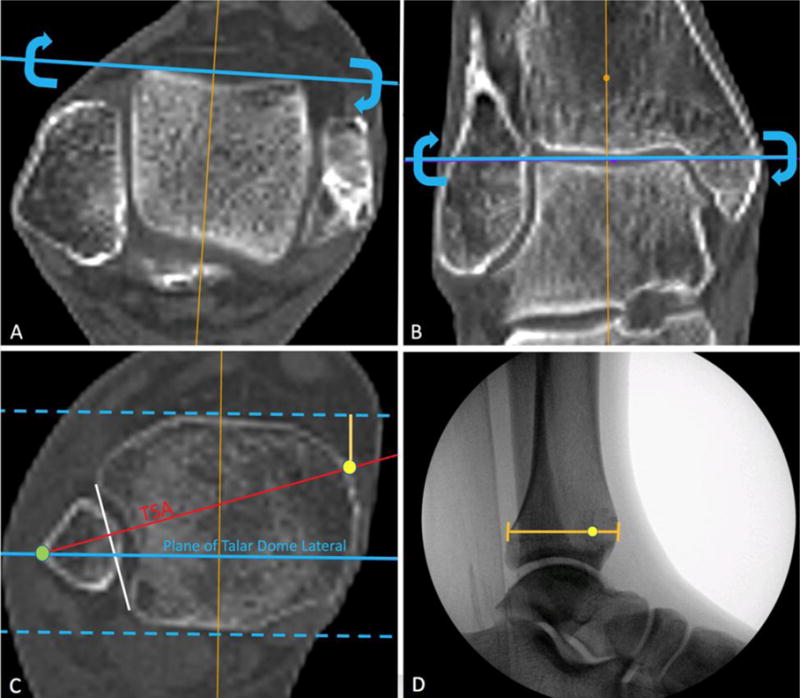
Objective: To describe a novel technique using preoperative computed tomography (CT) to plan clamp tine placement along the trans-syndesmotic axis (TSA). We hypothesized that preoperative CT imaging provides a reliable template on which to plan optimal clamp tine positioning along the TSA, reducing malreduction rates compared with other described techniques.
Methods: CT images of 48 cadaveric through-knee specimens were obtained, and the TSA was measured as well as the optimal position of the medial clamp tine. The syndesmosis was then fully destabilized. Indirect clamp reductions were performed with the medial clamp tine placed at positions 10 degrees anterior to the TSA, along the TSA, and at both 10 and 20 degrees posterior to the TSA. The specimens were then separately reduced using manual digital pressure and palpation alone. CT was performed after each clamp and manual reduction.
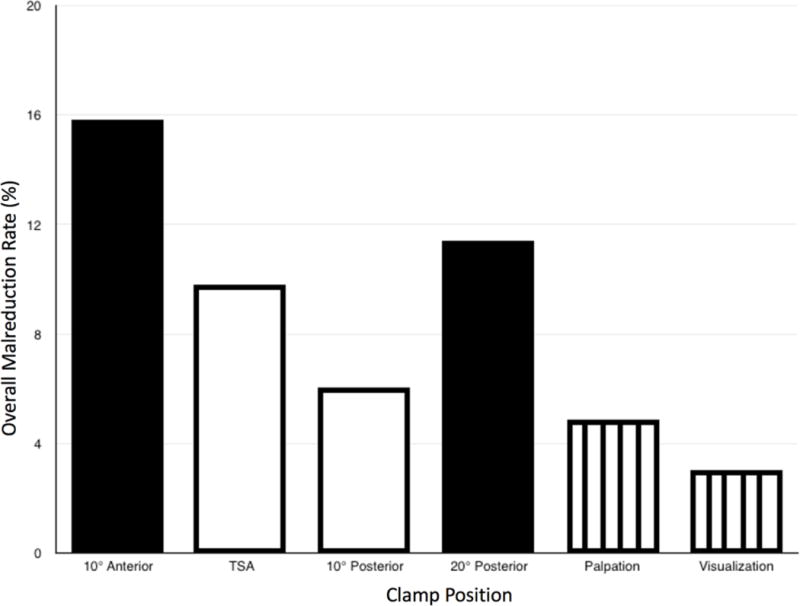
Results: On average, reduction clamp tines were within 3 ± 2 degrees of the desired angle and within 5% ± 4% of the templated location along the tibial line for all clamp reduction attempts. Palpation and direct visualization produced the overall lowest malreduction rates in all measurements: 4.9% and 3.0%, respectively. Off-axis clamping 10 degrees anterior or 20 degrees posterior to the patient-specific TSA demonstrated an increased overall malreduction rate: 15.8% and 11.3%, respectively. Significantly more over-compression occurred when a reduction clamp was used versus manual digital reduction alone (8.6% vs. 0%).
Conclusions: Reduction clamp placement directly along an optimal clamping vector can be facilitated by preoperative CT measurements of the uninjured ankle. However, even in this setting, the use of reduction clamps increases the risk for syndesmotic malreduction and over-compression compared with manual digital reduction or direct visualization.
Figures
Comment in
-
Invited Commentary related to: A Novel Indirect Reduction Technique in Ankle Syndesmotic Injuries: A Cadaveric Study.J Orthop Trauma. 2018 Jul;32(7):367-368. doi: 10.1097/BOT.0000000000001202. J Orthop Trauma. 2018. PMID: 29916990 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
