

Cost-Effectiveness of Left Atrial Appendage Closure With the WATCHMAN Device Compared With Warfarin or Non-Vitamin K Antagonist Oral Anticoagulants for Secondary Prevention in Nonvalvular Atrial Fibrillation
- PMID: 29739915
- PMCID: PMC5976225
- DOI: 10.1161/STROKEAHA.117.018825
Cost-Effectiveness of Left Atrial Appendage Closure With the WATCHMAN Device Compared With Warfarin or Non-Vitamin K Antagonist Oral Anticoagulants for Secondary Prevention in Nonvalvular Atrial Fibrillation
Abstract
Background and purpose: Once a patient with atrial fibrillation experiences an embolic event, the risk of a recurrent event increases 2.6-fold. New treatments have emerged as viable treatment alternatives to warfarin for stroke risk reduction in secondary prevention populations. This analysis sought to assess the cost-effectiveness of left atrial appendage closure (LAAC) compared with warfarin and the non-vitamin K antagonist oral anticoagulants dabigatran 150 mg, apixaban and rivaroxaban in the prevention of stroke in nonvalvular atrial fibrillation patients with a prior stroke or transient ischemic attack.
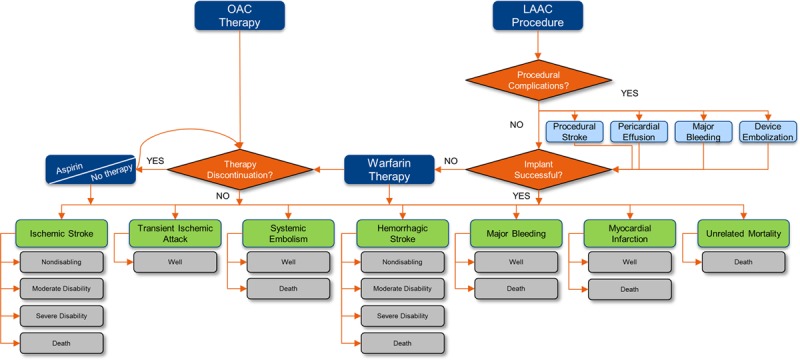
Methods: A Markov model was constructed using data from the secondary prevention subgroup analyses of the non-vitamin K antagonist oral anticoagulant and LAAC pivotal trials. Costs were from 2016 US Medicare reimbursement rates and the literature. The cost-effectiveness analysis was conducted from a US Medicare perspective over a lifetime (20 years) horizon. The model was populated with a cohort of 10 000 patients aged 70 years with a CHA2DS2-VASc score of 7 (annual stroke risk=9.60%) and HAS-BLED score of 3 (annual bleeding risk=3.74%).
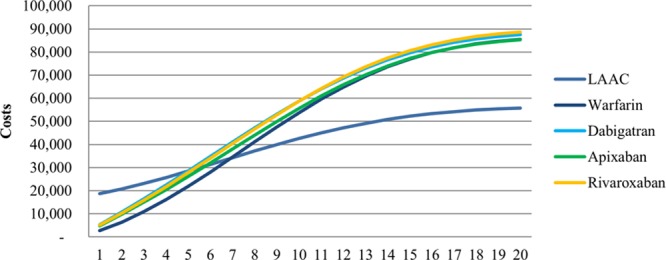
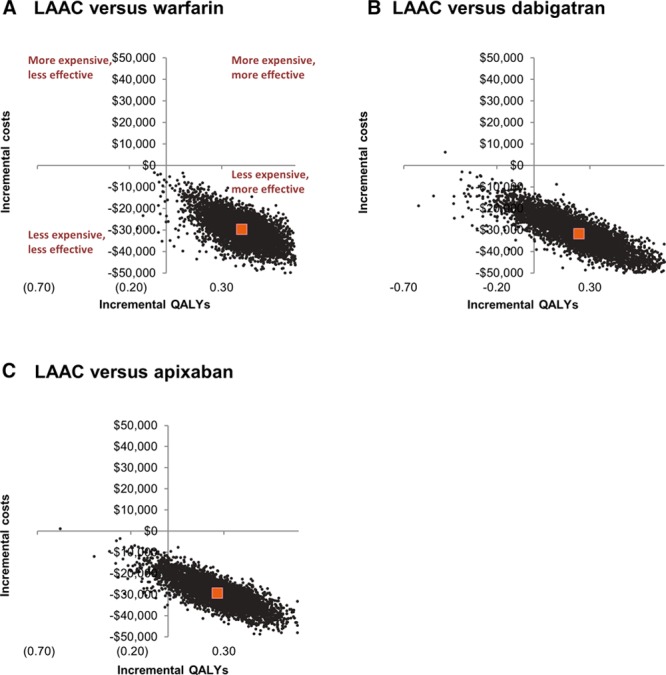
Results: LAAC achieved cost-effectiveness relative to dabigatran at year 5 and warfarin and apixaban at year 6. At 10 years, LAAC had more quality-adjusted life years (4.986 versus 4.769, 4.869, 4.888, and 4.810) and lower costs ($42 616 versus $53 770, $58 774, $55 656, and $58 655) than warfarin, dabigatran, apixaban, and rivaroxaban, respectively, making LAAC the dominant (more effective and less costly) stroke risk reduction strategy. LAAC remained the dominant strategy over the lifetime analysis.
Conclusions: Upfront procedure costs initially make LAAC higher cost than warfarin and the non-vitamin K antagonist oral anticoagulants, but within 10 years, LAAC delivers more quality-adjusted life years and has lower total costs, making LAAC the most cost-effective treatment strategy for secondary prevention of stroke in atrial fibrillation.
Keywords: apixaban; atrial fibrillation; cost-effectiveness analysis; dabigatran; left atrial appendage closure; warfarin.
© 2018 The Authors.
Figures
References
-
- Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31:2369–2429. - PubMed
-
- Stroke Prevention in Atrial Fibrillation Investigators. Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke Prevention in Atrial Fibrillation III randomised clinical trial. Lancet. 1996;348:633–638. doi: 10.1016/S0140-6736(96)03487-3. - PubMed
-
- European Atrial Fibrillation Trial (EAFT) Study Group. Secondary Prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255–1262. doi: 10.1016/0140-6736(93)92358-Z. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857e67. - PubMed
-
- Connelly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
