

A case of mixed adenoneuroendocrine carcinoma (MANEC) arising in Barrett's esophagus: literature and review
- PMID: 29740725
- PMCID: PMC5940966
- DOI: 10.1186/s40792-018-0454-z
A case of mixed adenoneuroendocrine carcinoma (MANEC) arising in Barrett's esophagus: literature and review
Abstract
Background: Mixed adenoneuroendocrine carcinoma (MANEC) is defined as a neoplasm composed of both exocrine and endocrine carcinomas, each comprising at least 30% of the tumor. MANEC can occur in various organs of the gastrointestinal tract, including the esophagus, stomach, and colon. We herein provide the first case report of surgically resected MANEC arising in Barrett's esophagus (BE).
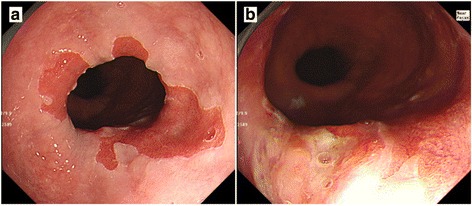
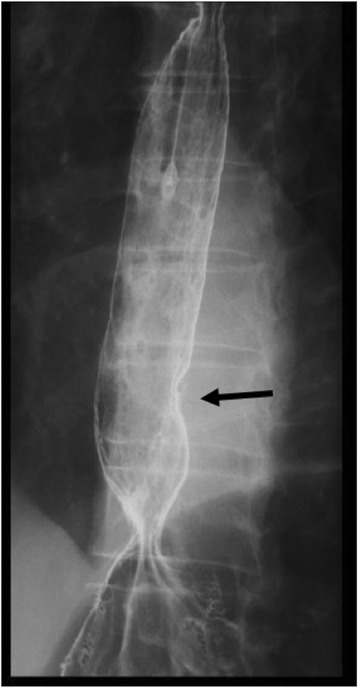
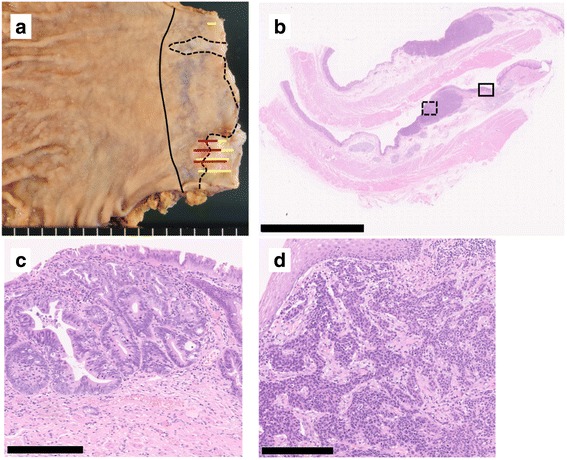
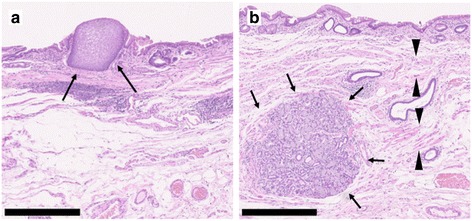
Case presentation: A 70-year-old man presenting with abdominal pain was referred to our hospital. Upper endoscopy showed a type 0-IIa + IIc elevated lesion adjacent to BE. According to a biopsy specimen, the elevated lesion was diagnosed as adenocarcinoma with neuroendocrine differentiation. No lymphatic or distant metastasis was detected in the preoperative examination. Laparoscopic distal esophagectomy and proximal gastrectomy were performed, and a diagnosis of MANEC in BE was determined according to the surgically resected specimen.
Conclusions: A very rare case of MANEC in BE was detected. BE can be the origin of esophageal MANEC as well as adenocarcinoma. Due to the small number of esophageal or esophagogastric MANEC cases reported, further accumulation of such cases is necessary to recommend an optimal management strategy for esophageal or esophagogastric MANEC.
Keywords: Barrett’s esophagus; Mixed adenoneuroendocrine carcinoma (MANEC); Neuroendocrine tumor.
Conflict of interest statement
Ethics approval and consent to participate
The present study was conducted in accordance with the ethical standards of our institution.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4th ed. Geneva: World Health Organization; 2010. https://www.cabdirect.org/cabdirect/abstract/20113051318.
LinkOut - more resources
Full Text Sources
Other Literature Sources
