

Behavioral Economics Interventions to Improve Outpatient Antibiotic Prescribing for Acute Respiratory Infections: a Cost-Effectiveness Analysis
- PMID: 29740788
- PMCID: PMC6544688
- DOI: 10.1007/s11606-018-4467-x
Behavioral Economics Interventions to Improve Outpatient Antibiotic Prescribing for Acute Respiratory Infections: a Cost-Effectiveness Analysis
Abstract
Background: Behavioral economics interventions have been shown to effectively reduce the rates of inappropriate antibiotic prescriptions for acute respiratory infections (ARIs).
Objective: To determine the cost-effectiveness of three behavioral economic interventions designed to reduce inappropriate antibiotic prescriptions for ARIs.
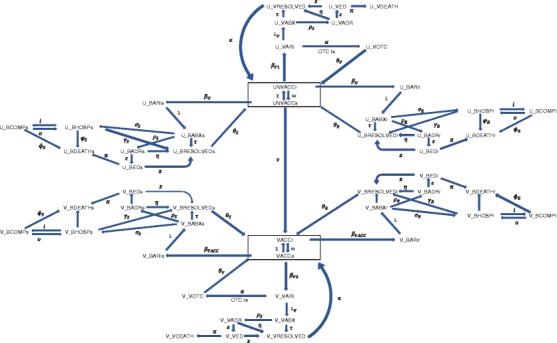
Design: Thirty-year Markov model from the US societal perspective with inputs derived from the literature and CDC surveillance data.
Subjects: Forty-five-year-old adults with signs and symptoms of ARI presenting to a healthcare provider.
Interventions: (1) Provider education on guidelines for the appropriate treatment of ARIs; (2) Suggested Alternatives, which utilizes computerized clinical decision support to suggest non-antibiotic treatment choices in lieu of antibiotics; (3) Accountable Justification, which mandates free-text justification into the patient's electronic health record when antibiotics are prescribed; and (4) Peer Comparison, which sends a periodic email to prescribers about his/her rate of inappropriate antibiotic prescribing relative to clinician colleagues.
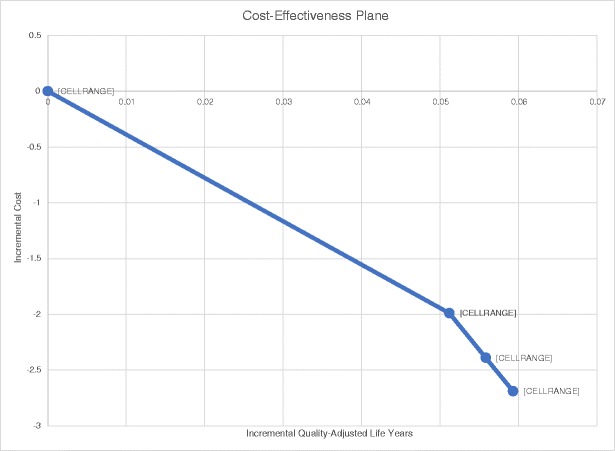
Main measures: Discounted costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios.
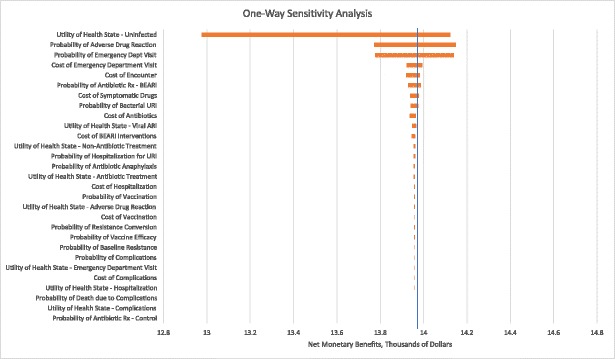
Key results: Each intervention has lower costs but higher QALYs compared to provider education. Total costs for each intervention were $178.21, $173.22, $172.82, and $172.52, and total QALYs were 14.68, 14.73, 14.74, and 14.74 for the control, Suggested Alternatives, Accountable Justification, and Peer Comparison groups, respectively. Results were most sensitive to the quality-of-life of the uninfected state, and the likelihood and costs for antibiotic-associated adverse events.
Conclusions: Behavioral economics interventions can be cost-effective strategies for reducing inappropriate antibiotic prescriptions by reducing healthcare resource utilization.
Trial registration: ClinicalTrials.gov NCT01454947.
Keywords: cost-effectiveness; healthcare administration; infectious disease; physician behavior.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Comment in
-
So Many Nudges, So Little Time: Can Cost-effectiveness Tell Us When It Is Worthwhile to Try to Change Provider Behavior?J Gen Intern Med. 2019 Jun;34(6):783-784. doi: 10.1007/s11606-019-04871-5. J Gen Intern Med. 2019. PMID: 30877456 Free PMC article. No abstract available.
References
-
- Llop CJ, Tuttle E, Tillotson GS, LaPlante K, File TM, Jr. Antibiotic treatment patterns, costs, and resource utilization among patients with community acquired pneumonia: a US cohort study. Hosp Pract (1995). 2017;1–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
