

The magnitude of obesity and metabolic syndrome among diabetic chronic kidney disease population: A nationwide study
- PMID: 29742114
- PMCID: PMC5942778
- DOI: 10.1371/journal.pone.0196332
The magnitude of obesity and metabolic syndrome among diabetic chronic kidney disease population: A nationwide study
Abstract
Background: Although the prevalence of obesity and metabolic syndrome (MetS) among dialysis patients has been exceeding than general population, little is known regarding obesity and MetS in non-dialysis chronic kidney disease (CKD). We aimed to find the magnitude of obesity and MetS and their associations with impaired renal function among type 2 diabetes mellitus (T2DM) patients.
Methods: A national survey of T2DM patients was collected in the Thai National Health Security Office database during 2014-5. The sampling frame was designated as distinct geographic regions throughout the country. A stratified two-stage cluster sampling was used to select the study population. Anthropometry and 12-hour fasting blood samples were obtained by trained personnel. BMI of ≥25 kg/m2 was classified as obesity. MetS was defined as having elevated waist circumference (>90 and >80 cm in men and women, respectively) plus any two of the followings: triglyceride ≥150 mg/dL, HDL-C <40 in men or <50 mg/dL in women, blood pressure ≥130/85 mmHg, and fasting blood sugar ≥100 mg/dL. CKD was defined as an impaired renal function (eGFR <60 mL/min/1.73m2 according to the CKD-EPI equation). Logistic regression analysis was performed to examine the relationship between obesity and MetS with the presence of CKD.
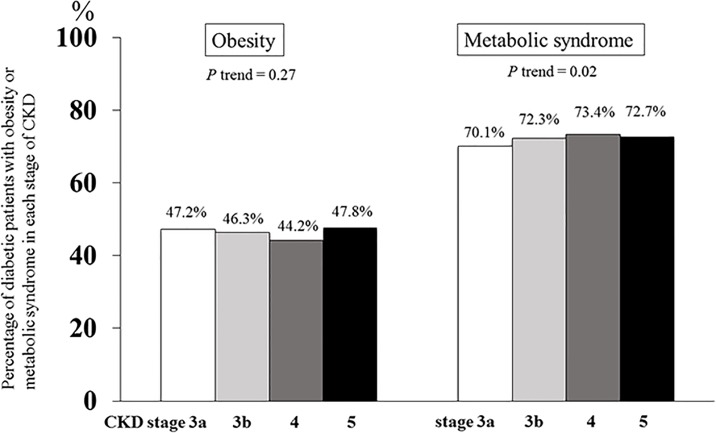
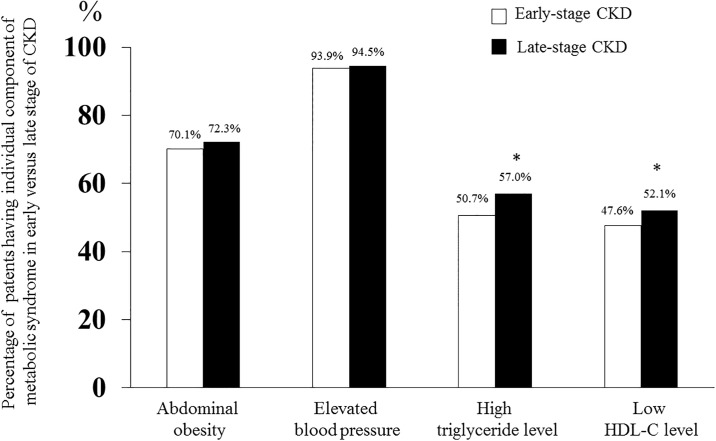
Results: A total of 32,616 diabetic patients were finally recruited from 997 hospitals. The mean age was 61.5±10.9 years with 67.5% women. Of the participants, 35.4% were CKD patients. The prevalence of obesity was 46.5% in CKD and 54.1% in non-CKD patients with T2DM (p<0.001). In contrast, the prevalence of MetS in CKD patients was higher than their non-CKD counterparts (71.3 vs 68.8%, p<0.001). Moreover, there was an association between the prevalence of MetS with CKD stage from 3a to 5 (70.1, 72.3, 73.4, and 72.7%, respectively, p trend = 0.02). MetS, but not obesity, had a significant association with CKD in T2DM patients after adjusting for age, sex, and comorbidities [OR 1.14; 95% CI 1.06-1.22, p<0.001]. When stratified by each component of MetS, only high serum triglyceride and low HDL-C levels were increased in patients with CKD stage 4 and 5 compared with CKD stage 3 (p<0.001) and had a significant relationship with impaired renal function.
Conclusion: There were relatively high prevalences of both obesity and MetS in T2DM patients. A higher prevalence of MetS, but lower prevalence of obesity, was observed among diabetic CKD group compared with their non-CKD counterparts. MetS, as a surrogate of insulin resistance, appeared to be more important than obesity in the development of impaired renal function in diabetic population.
Conflict of interest statement
Figures
Similar articles
-
Chronic Kidney Disease in Non-Diabetic Older Adults: Associated Roles of the Metabolic Syndrome, Inflammation, and Insulin Resistance.PLoS One. 2015 Oct 2;10(10):e0139369. doi: 10.1371/journal.pone.0139369. eCollection 2015. PLoS One. 2015. PMID: 26431218 Free PMC article.
-
Association between metabolic syndrome and chronic kidney disease in a Chinese urban population.Clin Chim Acta. 2017 Jul;470:103-108. doi: 10.1016/j.cca.2017.05.012. Epub 2017 May 10. Clin Chim Acta. 2017. PMID: 28501388
-
The association between metabolic syndrome components, low-grade systemic inflammation and insulin resistance in non-diabetic Indonesian adolescent male.Clin Nutr ESPEN. 2020 Feb;35:69-74. doi: 10.1016/j.clnesp.2019.12.001. Epub 2020 Jan 1. Clin Nutr ESPEN. 2020. PMID: 31987123
-
Metabolic syndrome and its components in premenopausal and postmenopausal women: a comprehensive systematic review and meta-analysis on observational studies.Menopause. 2018 Oct;25(10):1155-1164. doi: 10.1097/GME.0000000000001136. Menopause. 2018. PMID: 29787477
-
Effect of vegetarian diets on the presentation of metabolic syndrome or its components: A systematic review and meta-analysis.Clin Nutr. 2019 Jun;38(3):1117-1132. doi: 10.1016/j.clnu.2018.05.021. Epub 2018 Jun 6. Clin Nutr. 2019. PMID: 29907356
Cited by
-
Status of Nutrition In Hemodialysis Patients Survey (SNIPS): Malnutrition risk by diabetes status.Diabet Med. 2021 Jun;38(6):e14543. doi: 10.1111/dme.14543. Epub 2021 Feb 24. Diabet Med. 2021. PMID: 33583032 Free PMC article.
-
Prognostic value of metabolic syndrome in renal structural changes in type 2 diabetes.Int Urol Nephrol. 2022 Aug;54(8):2005-2014. doi: 10.1007/s11255-021-03051-x. Epub 2022 Jan 19. Int Urol Nephrol. 2022. PMID: 35043385
-
Water extract from processed Polygonum multiflorum modulate gut microbiota and glucose metabolism on insulin resistant rats.BMC Complement Med Ther. 2020 Apr 5;20(1):107. doi: 10.1186/s12906-020-02897-5. BMC Complement Med Ther. 2020. PMID: 32248799 Free PMC article.
-
Gut microbiota-derived SCFAs and MetS-related nephropathy.Front Nutr. 2025 Jul 8;12:1561271. doi: 10.3389/fnut.2025.1561271. eCollection 2025. Front Nutr. 2025. PMID: 40697558 Free PMC article. Review.
-
FIB-4 Index and Diabetes Mellitus Are Associated with Chronic Kidney Disease in Japanese Patients with Non-Alcoholic Fatty Liver Disease.Int J Mol Sci. 2019 Dec 25;21(1):171. doi: 10.3390/ijms21010171. Int J Mol Sci. 2019. PMID: 31881781 Free PMC article.
References
-
- World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation 2000, WHO Technical Report Series 894. Access date 22 Feb 2018. http://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/. - PubMed
-
- Subramanian SV, Perkins JM, Ozaltin E, Davey Smith G. Weight of nations: a socioeconomic analysis of women in low- to middle-income countries. Am J Clin Nutr 2011;93:413–421. doi: 10.3945/ajcn.110.004820 - DOI - PMC - PubMed
-
- Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003;289:76–79. - PubMed
-
- Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 2002;287:356–359. - PubMed
-
- Obermayr RP, Temml C, Knechtelsdorfer M, Gutjahr G, Kletzmayr J, Heiss S, et al. Predictors of new-onset decline in kidney function in a general middle-european population. Nephrol Dial Transplant 2008;23:1265–1273. doi: 10.1093/ndt/gfm790 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
