

Binding of Free and Immune Complex-Associated Hepatitis C Virus to Erythrocytes Is Mediated by the Complement System
- PMID: 29742812
- PMCID: PMC6226377
- DOI: 10.1002/hep.30087
Binding of Free and Immune Complex-Associated Hepatitis C Virus to Erythrocytes Is Mediated by the Complement System
Abstract
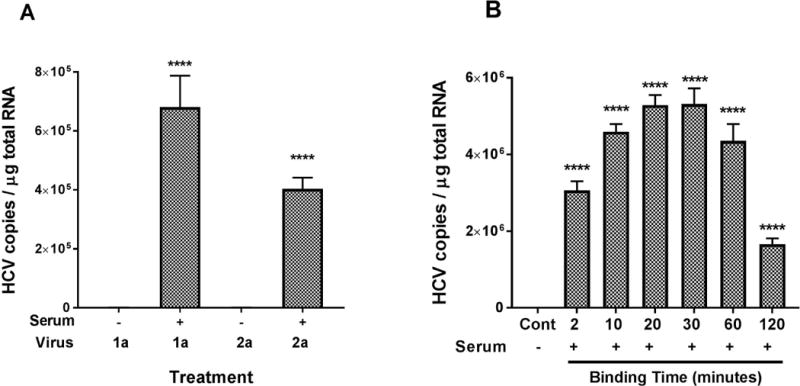
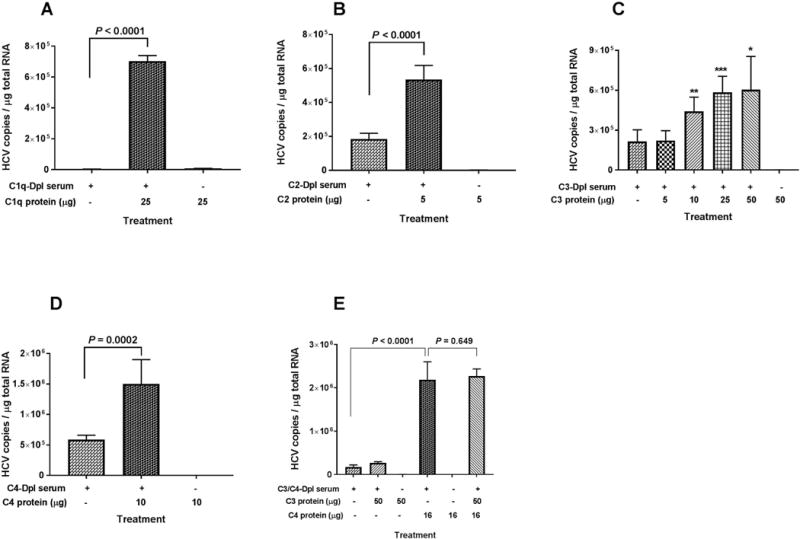
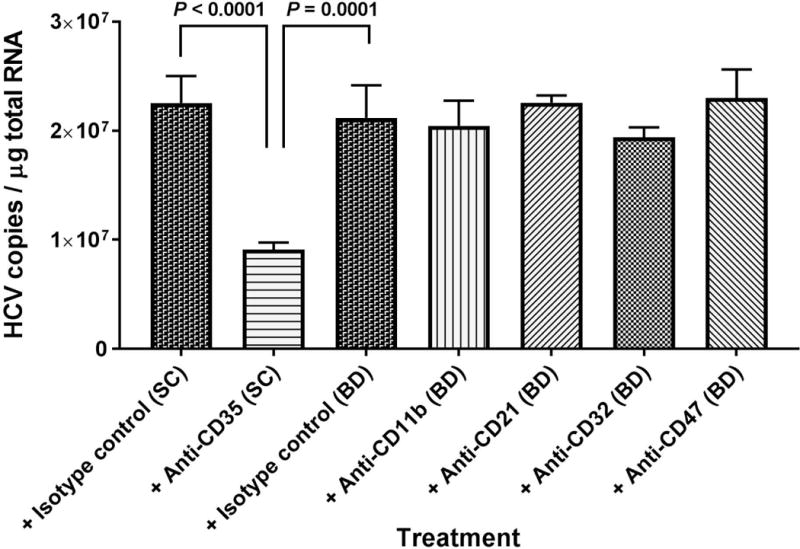
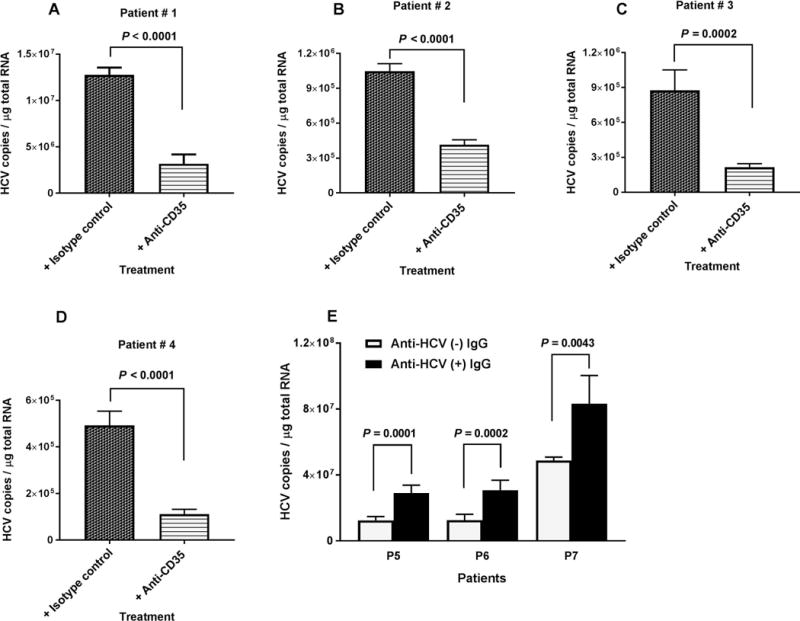
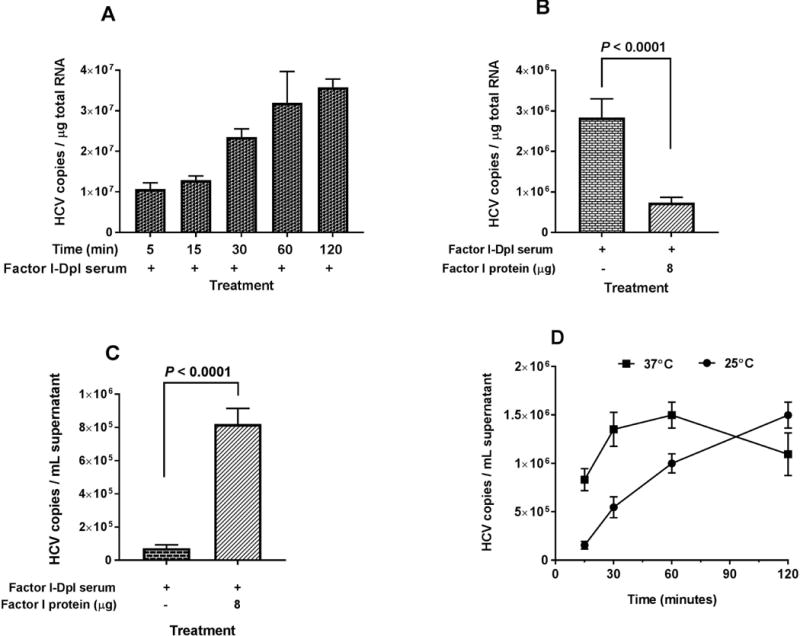
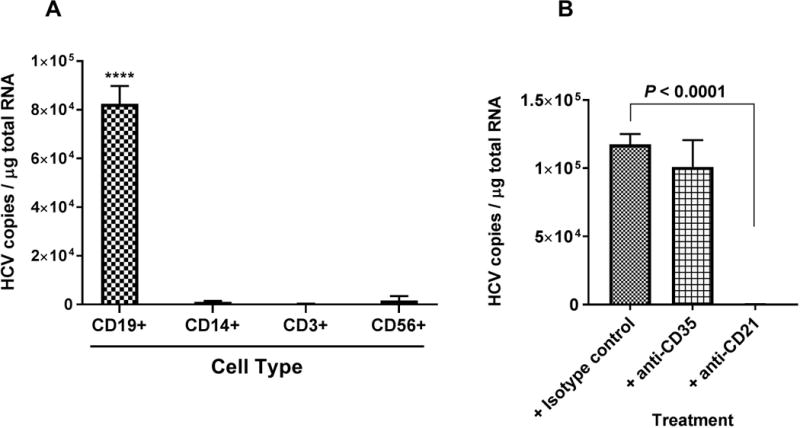
Erythrocytes bind circulating immune complexes (ICs) and facilitate IC clearance from the circulation. Chronic hepatitis C virus (HCV) infection is associated with IC-related disorders. In this study, we investigated the kinetics and mechanism of HCV and HCV-IC binding to and dissociation from erythrocytes. Cell culture-produced HCV was mixed with erythrocytes from healthy blood donors, and erythrocyte-associated virus particles were quantified. Purified complement proteins, complement-depleted serum, and complement receptor antibodies were used to investigate complement-mediated HCV-erythrocyte binding. Purified HCV-specific immunoglobulin G (IgG) from a chronic HCV-infected patient was used to study complement-mediated HCV-IC/erythrocyte binding. Binding of HCV to erythrocytes increased 200- to 1,000-fold after adding complement active human serum in the absence of antibody. Opsonization of free HCV occurred within 10 minutes, and peak binding to erythrocytes was observed at 20-30 minutes. Complement protein C1 was required for binding, whereas C2, C3, and C4 significantly enhanced binding. Complement receptor 1 (CR1, CD35) antibodies blocked the binding of HCV to erythrocytes isolated from chronically infected HCV patients and healthy blood donors. HCV-ICs significantly enhanced complement-mediated binding to erythrocytes compared to unbound HCV. Dissociation of complement-opsonized HCV from erythrocytes depended on the presence of Factor I. HCV released by Factor I bound preferentially to CD19+ B cells compared to other leukocytes. Conclusion: These results demonstrate that complement mediates the binding of free and IC-associated HCV to CR1 on erythrocytes and provide a mechanistic rationale for investigating the differential phenotypic expression of HCV-IC-related disease.
Published 2018. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
Potential conflict of interest: Nothing to report.
Figures
References
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57:1333–1342. - PubMed
-
- Burra P, De Martin E, Zanetto A, Senzolo M, Russo FP, Zanus G, Fagiuoli S. Hepatitis C virus and liver transplantation: where do we stand? Transpl Int. 2016;29:135–152. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
