

Predictive biomarkers for death and rehospitalization in comorbid frail elderly heart failure patients
- PMID: 29743019
- PMCID: PMC5944009
- DOI: 10.1186/s12877-018-0807-2
Predictive biomarkers for death and rehospitalization in comorbid frail elderly heart failure patients
Abstract
Background: Heart failure (HF) is associated with a high rate of readmissions within 30 days post-discharge and in the following year, especially in frail elderly patients. Biomarker data are scarce in this high-risk population. This study assessed the value of early post-discharge circulating levels of ST2, NT-proBNP, CA125, and hs-TnI for predicting 30-day and 1-year outcomes in comorbid frail elderly patients with HF with mainly preserved ejection fraction (HFpEF).
Methods: Blood samples were obtained at the first visit shortly after discharge (4.9 ± 2 days). The primary endpoint was the composite of all-cause mortality or HF-related rehospitalization at 30 days and at 1 year. All-cause mortality alone at one year was also a major endpoint. HF-related rehospitalizations alone were secondary end-points.
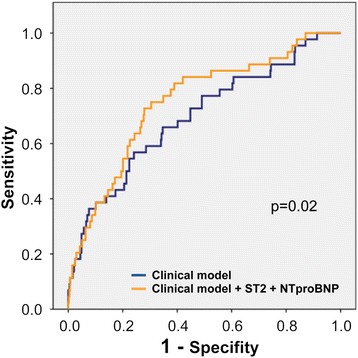
Results: From February 2014 to November 2016, 522 consecutive patients attending the STOP-HF Clinic were included (57.1% women, age 82 ± 8.7 years, mean Barthel index 70 ± 25, mean Charlson comorbidity index 5.6 ± 2.2). The composite endpoint occurred in 8.6% patients at 30 days and in 38.5% at 1 year. In multivariable analysis, ST2 [hazard ratio (HR) 1.53; 95% CI 1.19-1.97; p = 0.001] was the only predictive biomarker at 30 days; at 1 year, both ST2 (HR 1.34; 95% CI 1.15-1.56; p < 0.001) and NT-proBNP (HR 1.19; 95% CI 1.02-1.40; p = 0.03) remained significant. The addition of ST2 and NT-proBNP into a clinical predictive model increased the AUC from 0.70 to 0.75 at 30 days (p = 0.02) and from 0.71 to 0.74 at 1 year (p < 0.05). For all-cause death at 1 year, ST2 (HR 1.50; 95% CI 1.26-1.80; p < 0.001), and CA125 (HR 1.41; 95% CI 1.21-1.63; p < 0.001) remained independent predictors in multivariable analysis. The addition of ST2 and CA125 into a clinical predictive model increased the AUC from 0.74 to 0.78 (p = 0.03). For HF-related hospitalizations, ST2 was the only predictive biomarker in multivariable analyses, both at 30 days and at 1 year.
Conclusions: In a comorbid frail elderly population with HFpEF, ST2 outperformed NT-proBNP for predicting the risk of all-cause mortality or HF-related rehospitalization. ST2, a surrogate marker of inflammation and fibrosis, may be a better predictive marker in high-risk HFpEF.
Conflict of interest statement
Ethics approval and consent to participate
All participants provided written informed consent, and the study was approved by the local ethics committee (Comité Ètic de la Investigació de l’Hospital Universitari Germans Trias i Pujol; EO-10-076). All study procedures were performed in accordance with the ethical standards outlined in the Helsinki Declaration of 1975 as revised in 2013.
Competing interests
JL received lecture honoraria from Roche Diagnostics and reports a relationship with Critical Diagnostics.
JN received board membership fees and travel expenses from Novartis, Roche Diagnostics, Abbott, Rovi, and Vifor.
AB-G received board membership fees and travel expenses from Novartis and Roche Diagnostics and reports a relationship with Critical Diagnostics.
The rest of the authors have no disclosures to mention.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
