

Clinical Implications of Ablation of Drivers for Atrial Fibrillation: A Systematic Review and Meta-Analysis
- PMID: 29743170
- PMCID: PMC6474343
- DOI: 10.1161/CIRCEP.117.006119
Clinical Implications of Ablation of Drivers for Atrial Fibrillation: A Systematic Review and Meta-Analysis
Abstract
Background: The outcomes from pulmonary vein isolation (PVI) for atrial fibrillation (AF) are suboptimal, but the benefits of additional lesion sets remain unproven. Recent studies propose ablation of AF drivers improves outcomes over PVI, yet with conflicting reports in the literature. We undertook a systematic literature review and meta-analysis to determine outcomes from ablation of AF drivers in addition to PVI or as a stand-alone procedure.
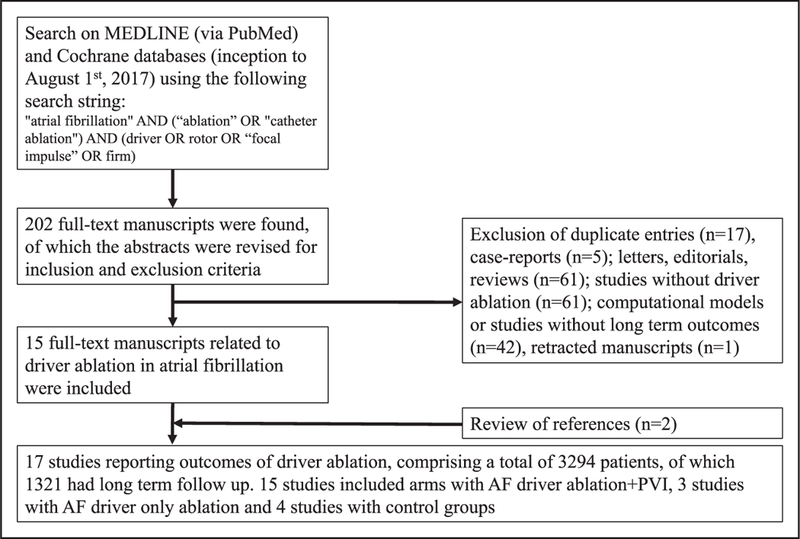
Methods: Database search was done using the terms atrial fibrillation and ablation or catheter ablation and driver or rotor or focal impulse or FIRM (Focal Impulse and Rotor Modulation). We pooled data using random effects model and assessed heterogeneity with I2 statistic.
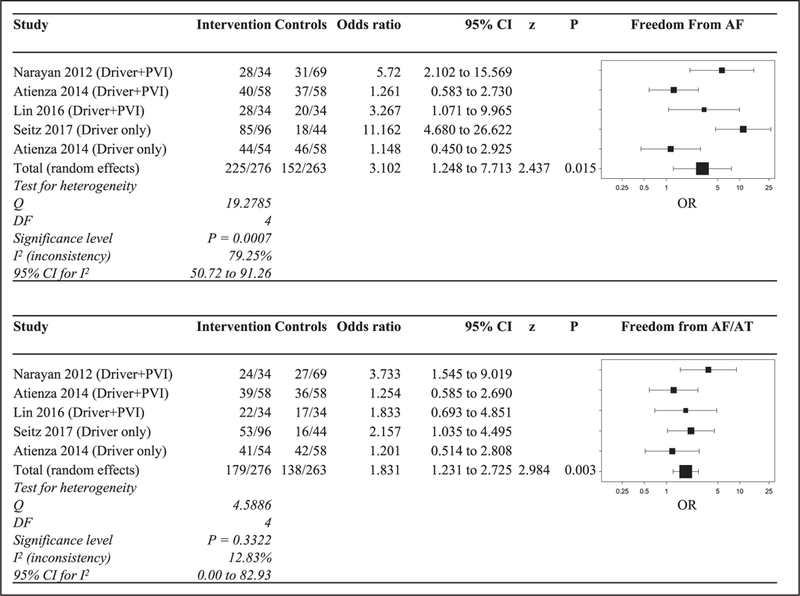
Results: Seventeen studies met inclusion criteria, in a cohort size of 3294 patients. Adding AF driver ablation to PVI reported freedom from AF of 72.5% (confidence interval [CI], 62.1%-81.8%; P<0.01) and from all arrhythmias of 57.8% (CI, 47.5%-67.7%; P<0.01). AF driver ablation when added to PVI or as stand-alone procedure compared with controls produced an odds ratio of 3.1 (CI, 1.3-7.7; P=0.02) for freedom from AF and an odds ratio of 1.8 (CI, 1.2-2.7; P<0.01) for freedom from all arrhythmias in 4 controlled studies. AF termination rate was 40.5% (CI, 30.6%-50.9%) and predicted favorable outcome from ablation(P<0.05).
Conclusions: In controlled studies, the addition of AF driver ablation to PVI supports the possible benefit of a combined approach of AF driver ablation and PVI in improving single-procedure freedom from all arrhythmias. However, most studies are uncontrolled and are limited by substantial heterogeneity in outcomes. Large multicenter randomized trials are needed to precisely define the benefits of adding driver ablation to PVI.
Keywords: ablation, catheter; arrhythmia; atrial fibrillation; cohort studies; freedom; meta-analysis; odds ratio.
© 2018 American Heart Association, Inc.
Conflict of interest statement
The other authors report no conflicts.
Figures


References
-
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, Chen PS, Chen SA, Chung MK, Nielsen JC, Curtis AB, Davies DW, Day JD, d’Avila A, de Groot NMSN, Di Biase L, Duytschaever M, Edgerton JR, Ellenbogen KA, Ellinor PT, Ernst S, Fenelon G, Gerstenfeld EP, Haines DE, Haissaguerre M, Helm RH, Hylek E, Jackman WM, Jalife J, Kalman JM, Kautzner J, Kottkamp H, Kuck KH, Kumagai K, Lee R, Lewalter T, Lindsay BD, Macle L, Mansour M, Marchlinski FE, Michaud GF, Nakagawa H, Natale A, Nattel S, Okumura K, Packer D, Pokushalov E, Reynolds MR, Sanders P, Scanavacca M, Schilling R, Tondo C, Tsao HM, Verma A, Wilber DJ, Yamane T. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14:e275–e444. doi: 10.1016/j.hrthm.2017.05.012. - DOI - PMC - PubMed
-
- Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, Macle L, Morillo CA, Haverkamp W, Weerasooriya R, Albenque JP, Nardi S, Menardi E, Novak P, Sanders P; STAR AF II Investigators. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–1822. doi: 10.1056/NEJMoa1408288. - DOI - PubMed
-
- Wong KC, Paisey JR, Sopher M, Balasubramaniam R, Jones M, Qureshi N, Hayes CR, Ginks MR, Rajappan K, Bashir Y, Betts TR. No benefit of complex fractionated atrial electrogram ablation in addition to circumferential pulmonary vein ablation and linear ablation: benefit of complex ablation study. Circ Arrhythm Electrophysiol. 2015;8:1316–1324. doi: 10.1161/CIRCEP.114.002504. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
