

Overlap between age-at-onset and disease-progression determinants in Huntington disease
- PMID: 29743208
- PMCID: PMC5996832
- DOI: 10.1212/WNL.0000000000005690
Overlap between age-at-onset and disease-progression determinants in Huntington disease
Abstract
Objective: A fundamental but still unresolved issue regarding Huntington disease (HD) pathogenesis is whether the factors that determine age at onset are the same as those that govern disease progression. Because elucidation of this issue is crucial for the development as well as optimal timing of administration of novel disease-modifying therapies, we aimed to assess the extent of overlap between age-at-onset and disease-progression determinants in HD.
Methods: Using observational data from Enroll-HD, the largest cohort of patients with HD worldwide, in this study we present, validate, and apply an intuitive method based on linear mixed-effect models to quantify the variability in the rate of disease progression in HD.
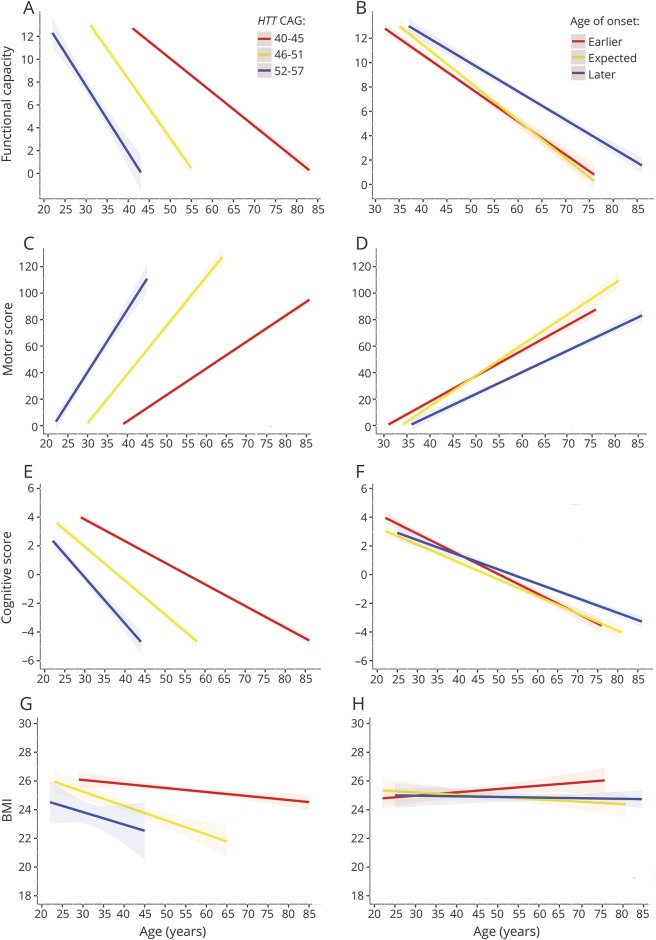
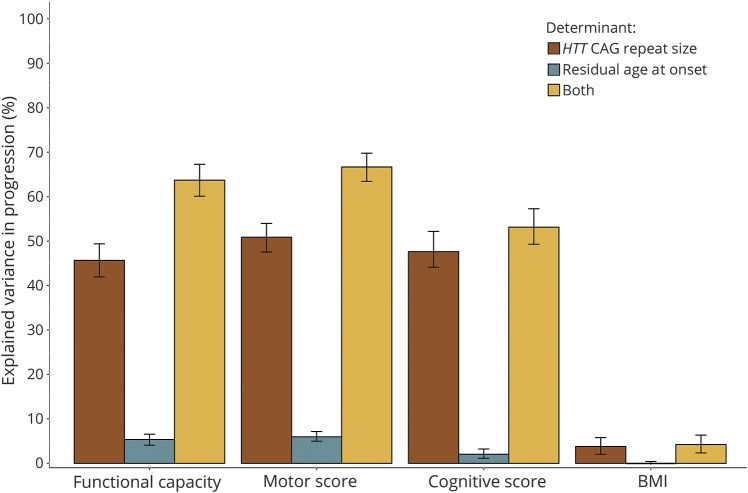
Results: A total of 3,411 patients with HD met inclusion criteria. We found that (1) about two-thirds of the rate of functional, motor, and cognitive progression in HD is determined by the same factors that also determine age at onset, with CAG repeat-dependent mechanisms having by far the largest effect; (2) although expanded HTT CAG repeat size had a large influence on average body weight, the rate of weight loss was largely independent of factors that determine age at onset in HD; and (3) about one-third of the factors that determine the rate of functional, motor, and cognitive progression are different from those that govern age at onset and need further elucidation.
Conclusion: Our findings imply that targeting of CAG repeat-dependent mechanisms, for example through gene-silencing approaches, is likely to affect the rate of functional, motor, and cognitive impairment, but not weight loss, in manifest HD mutation carriers.
© 2018 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Ameliorating the age at onset and disease progression in Huntington disease.Neurology. 2018 Jun 12;90(24):1087-1088. doi: 10.1212/WNL.0000000000005670. Epub 2018 May 9. Neurology. 2018. PMID: 29743206 No abstract available.
References
-
- The Huntington Disease Collaborative Research Group. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington's disease chromosomes. Cell 1993;72:971–983. - PubMed
-
- Walker FO. Huntington's disease. Lancet 2007;369:218–228. - PubMed
-
- Cazeneuve C, Durr A. Genetic and molecular studies. In: Bates GP, Tabrizi SJ, Jones L, editors. Huntington's Disease, 4th ed. New York: Oxford University Press; 2014:109–130.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous