

Is psychosis a multisystem disorder? A meta-review of central nervous system, immune, cardiometabolic, and endocrine alterations in first-episode psychosis and perspective on potential models
- PMID: 29743584
- PMCID: PMC6124651
- DOI: 10.1038/s41380-018-0058-9
Is psychosis a multisystem disorder? A meta-review of central nervous system, immune, cardiometabolic, and endocrine alterations in first-episode psychosis and perspective on potential models
Erratum in
-
Correction to: Is psychosis a multisystem disorder? A meta-review of central nervous system, immune, cardiometabolic, and endocrine alterations in first-episode psychosis and perspective on potential models.Mol Psychiatry. 2019 Jun;24(6):928. doi: 10.1038/s41380-018-0275-2. Mol Psychiatry. 2019. PMID: 30337658 Free PMC article.
Abstract
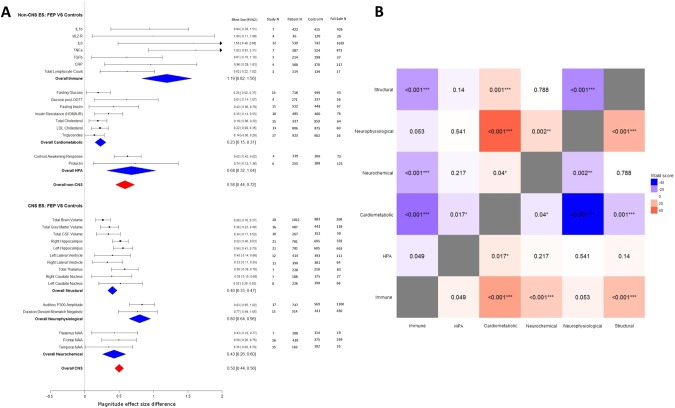
People with psychotic disorders show abnormalities in several organ systems in addition to the central nervous system (CNS); and this contributes to excess mortality. However, it is unclear how strong the evidence is for alterations in non-CNS systems at the onset of psychosis, how the alterations in non-CNS systems compare to those in the CNS, or how they relate to symptoms. Here, we consider these questions, and suggest potential models to account for findings. We conducted a systematic meta-review to summarize effect sizes for both CNS (focusing on brain structural, neurophysiological, and neurochemical parameters) and non-CNS dysfunction (focusing on immune, cardiometabolic, and hypothalamic-pituitary-adrenal (HPA) systems) in first-episode psychosis (FEP). Relevant meta-analyses were identified in a systematic search of Pubmed and the methodological quality of these was assessed using the AMSTAR checklist (A Measurement Tool to Assess Systematic Reviews). Case-control data were extracted from studies included in these meta-analyses. Random effects meta-analyses were re-run and effect size magnitudes for individual parameters were calculated, as were summary effect sizes for each CNS and non-CNS system. We also grouped studies to obtain overall effect sizes for non-CNS and CNS alterations. Robustness of data for non-CNS and CNS parameters was assessed using Rosenthal's fail-safe N. We next statistically compared summary effect size for overall CNSand overall non-CNS alterations, as well as for each organ system separately. We also examined how non-CNS alterations correlate CNS alterations, and with psychopathological symptoms. Case-control data were extracted for 165 studies comprising a total sample size of 13,440. For people with first episode psychosis compared with healthy controls, we observed alterations in immune parameters (summary effect size: g = 1.19), cardiometabolic parameters (g = 0.23); HPA parameters (g = 0.68); brain structure (g = 0.40); neurophysiology (g = 0.80); and neurochemistry (g = 0.43). Grouping non-CNS organ systems together provided an effect size for overall non-CNS alterations in patients compared with controls (g = 0.58), which was not significantly different from the overall CNS alterations effect size (g = 0.50). However, the summary effect size for immune alterations was significantly greater than that for brain structural (P < 0.001) and neurochemical alterations (P < 0.001), while the summary effect size for cardiometabolic alterations was significantly lower than neurochemical (P = 0.04), neurophysiological (P < 0.001), and brain structural alterations (P = 0.001). The summary effect size for HPA alterations was not significantly different from brain structural (P = 0.14), neurophysiological (P = 0.54), or neurochemical alterations (P = 0.22). These outcomes remained similar in antipsychotic naive sensitivity analyses. We found some, but limited and inconsistent, evidence that non-CNS alterations were associated with CNS changes and symptoms in first episode psychosis. Our findings indicate that there are robust alterations in non-CNS systems in psychosis, and that these are broadly similar in magnitude to a range of CNS alterations. We consider models that could account for these findings and discuss implications for future research and treatment.
Figures

References
-
- Saha S, Chant D, McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry. 2007;64:1123–31. - PubMed
-
- Whiteford HA, Baxter AJ. The Global Burden of Disease 2010 Study: what does it tell us about mental disorders in Latin America? Rev Bras Psiquiatr. 2013;35:111–2. - PubMed
-
- Knapp M, Mangalore R, Simon J. The global costs of schizophrenia. Schizophr Bull. 2004;30:279–93. - PubMed
-
- Crump C, Winkleby MA, Sundquist K, Sundquist J. Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am J Psychiatry. 2013;170:324–33. - PubMed
-
- Hoang U, Goldacre MJ, Stewart R. Avoidable mortality in people with schizophrenia or bipolar disorder in England. Acta Psychiatr Scand. 2013;127:195–201. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
