

Bone grafts and biomaterials substitutes for bone defect repair: A review
- PMID: 29744432
- PMCID: PMC5935655
- DOI: 10.1016/j.bioactmat.2017.05.007
Bone grafts and biomaterials substitutes for bone defect repair: A review
Abstract
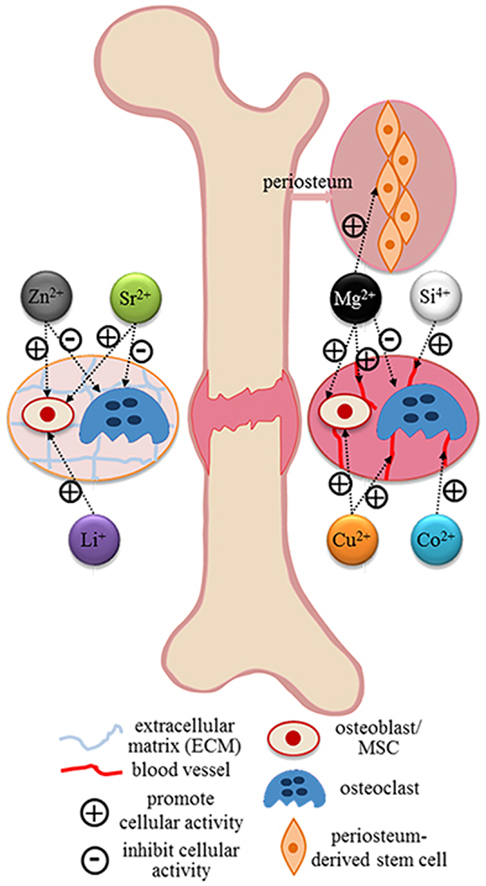
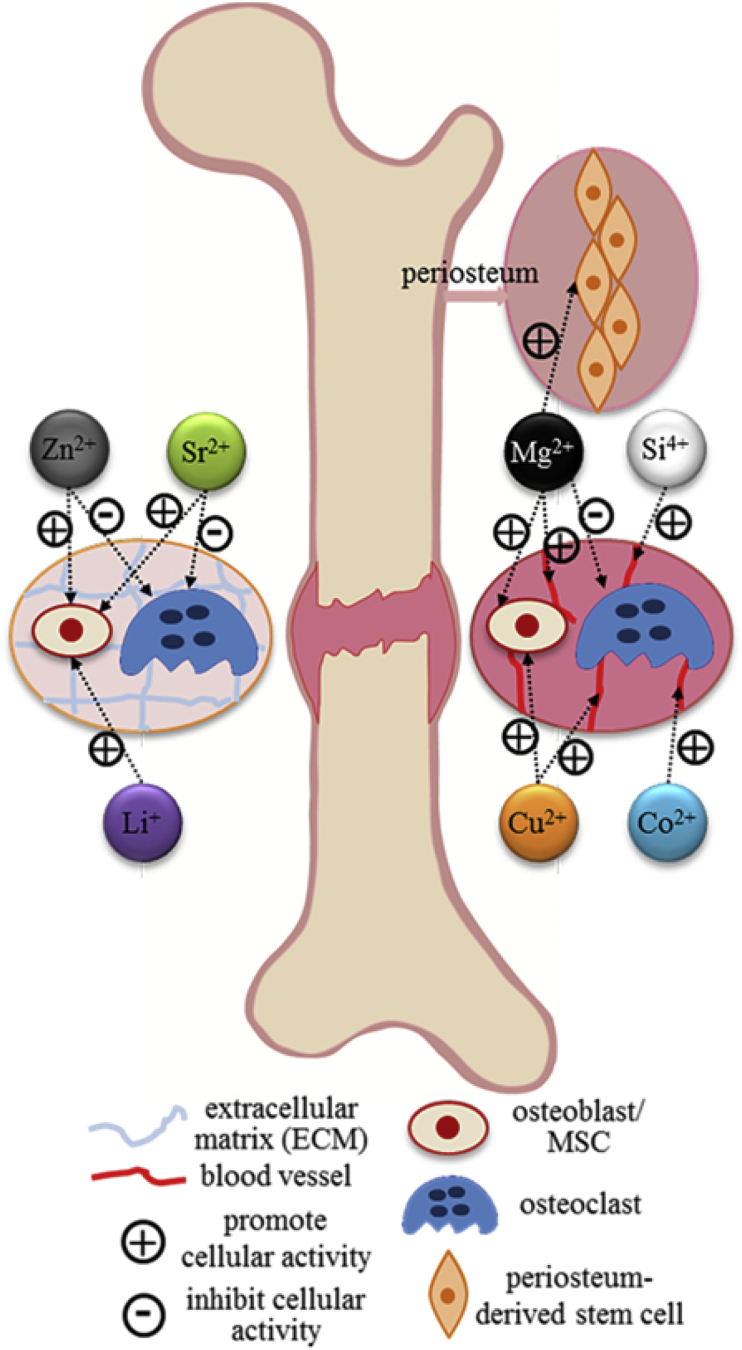
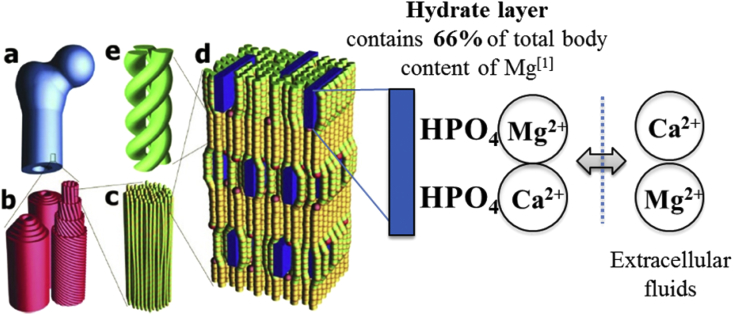
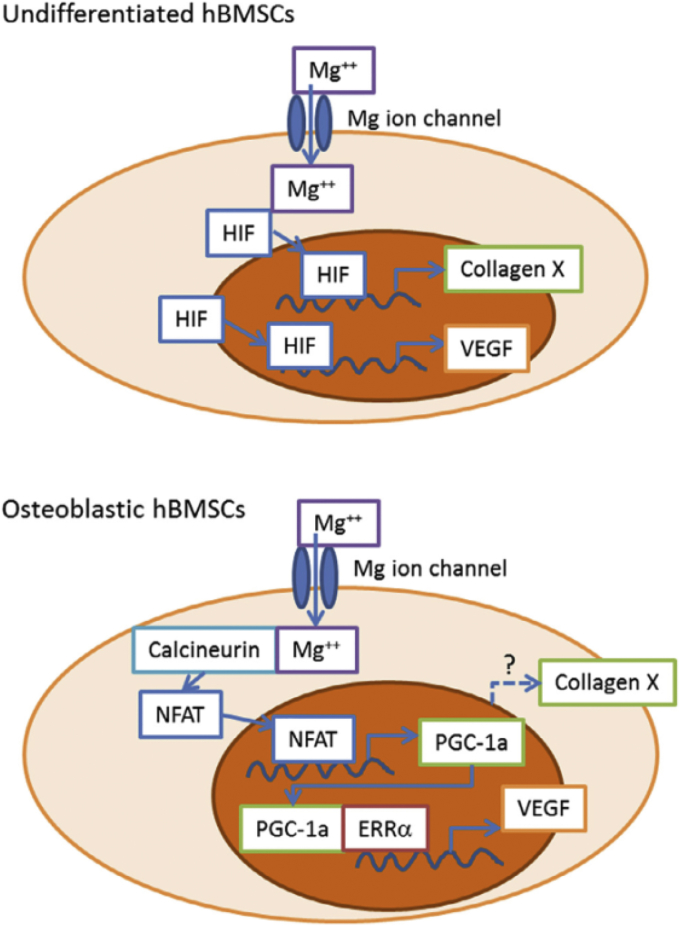
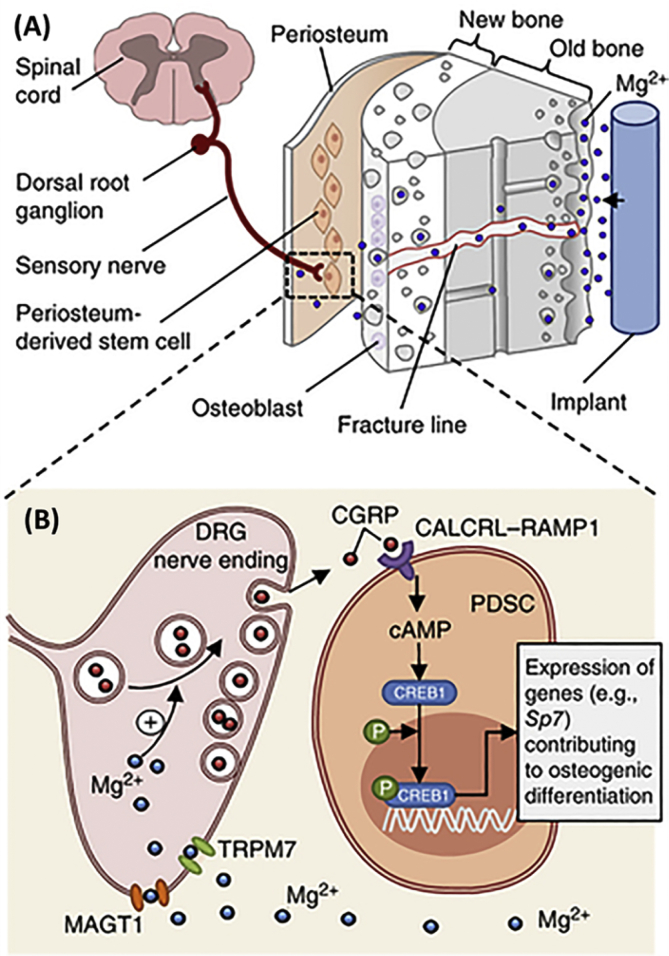
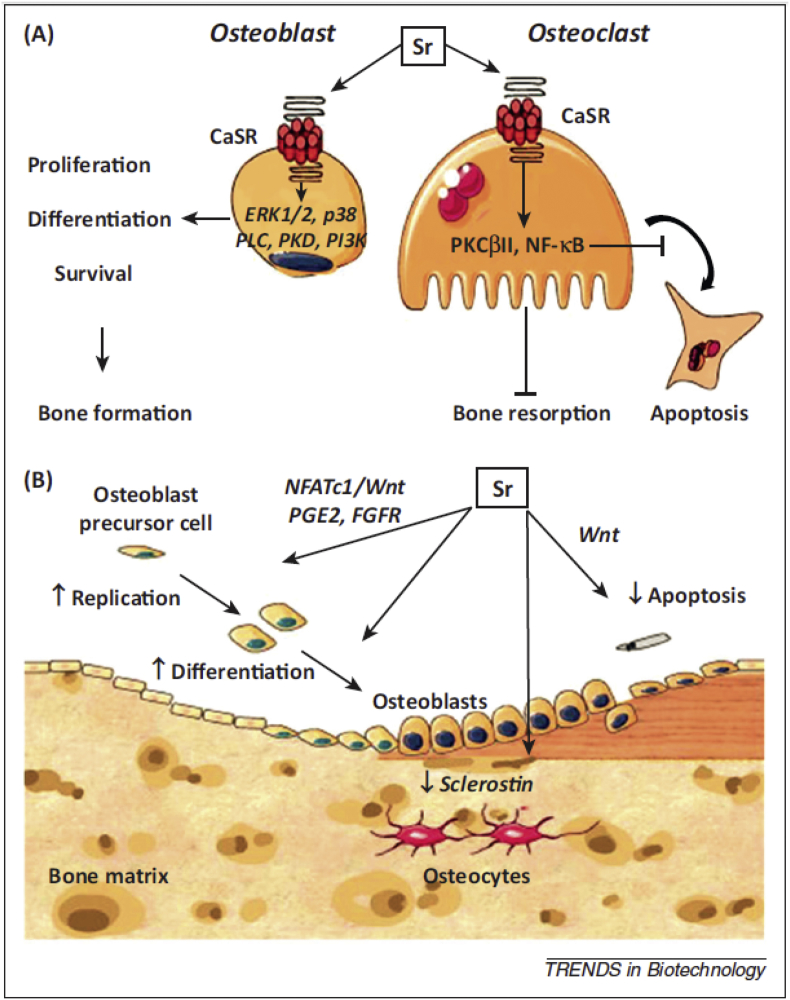
Bone grafts have been predominated used to treat bone defects, delayed union or non-union, and spinal fusion in orthopaedic clinically for a period of time, despite the emergency of synthetic bone graft substitutes. Nevertheless, the integration of allogeneic grafts and synthetic substitutes with host bone was found jeopardized in long-term follow-up studies. Hence, the enhancement of osteointegration of these grafts and substitutes with host bone is considerably important. To address this problem, addition of various growth factors, such as bone morphogenetic proteins (BMPs), parathyroid hormone (PTH) and platelet rich plasma (PRP), into structural allografts and synthetic substitutes have been considered. Although clinical applications of these factors have exhibited good bone formation, their further application was limited due to high cost and potential adverse side effects. Alternatively, bioinorganic ions such as magnesium, strontium and zinc are considered as alternative of osteogenic biological factors. Hence, this paper aims to review the currently available bone grafts and bone substitutes as well as the biological and bio-inorganic factors for the treatments of bone defect.
Keywords: Bioinorganic ions; Bone grafts and substitutes; Fracture healing; Growth factors.
Figures
References
-
- Bhatt R.A., Rozental T.D. Bone graft substitutes. Hand Clin. 2012;28:457–468. - PubMed
-
- Greenwald A.S., Boden S.D., Goldberg V.M., Yaszemski M., Heim C.S. Bone-graft Substitutes: Facts, Fictions and Applications, AAOS 75th Annual Meeting. 2008. - PubMed
-
- Bauer T.W., Muschler G.F. Bone graft materials: an overview of the basic science. Clin. Orthop. Relat. Res. 2000;371:10–27. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
