

Free water modeling of peritumoral edema using multi-fiber tractography: Application to tracking the arcuate fasciculus for neurosurgical planning
- PMID: 29746544
- PMCID: PMC5944935
- DOI: 10.1371/journal.pone.0197056
Free water modeling of peritumoral edema using multi-fiber tractography: Application to tracking the arcuate fasciculus for neurosurgical planning
Abstract
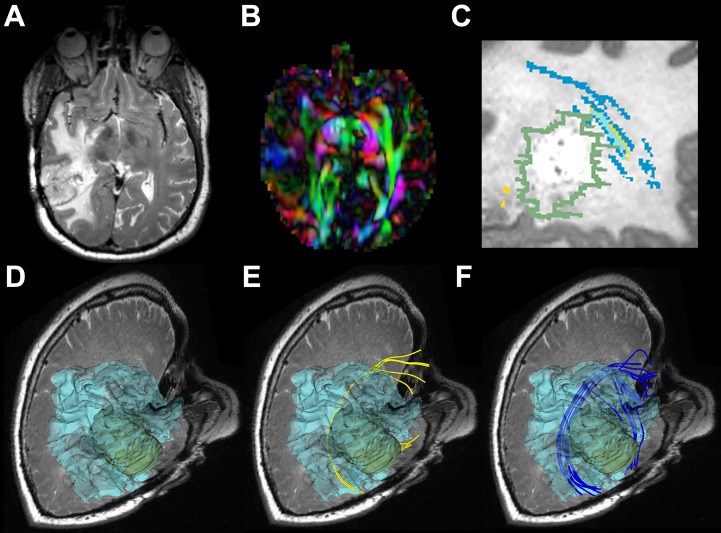
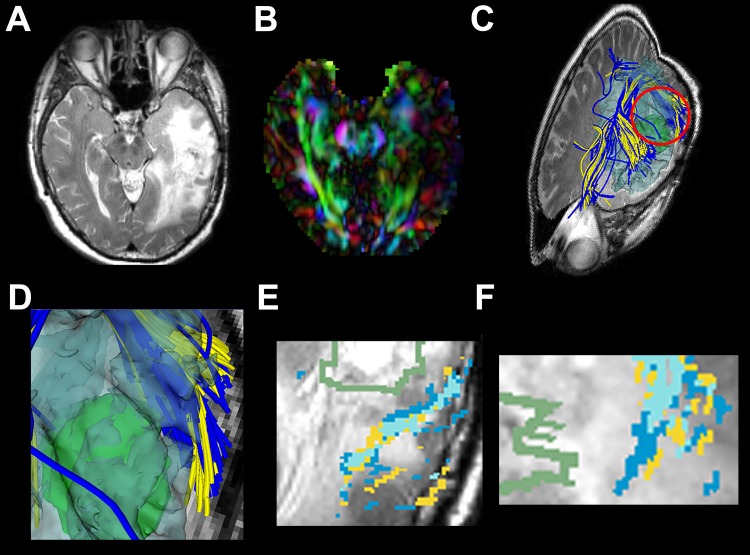
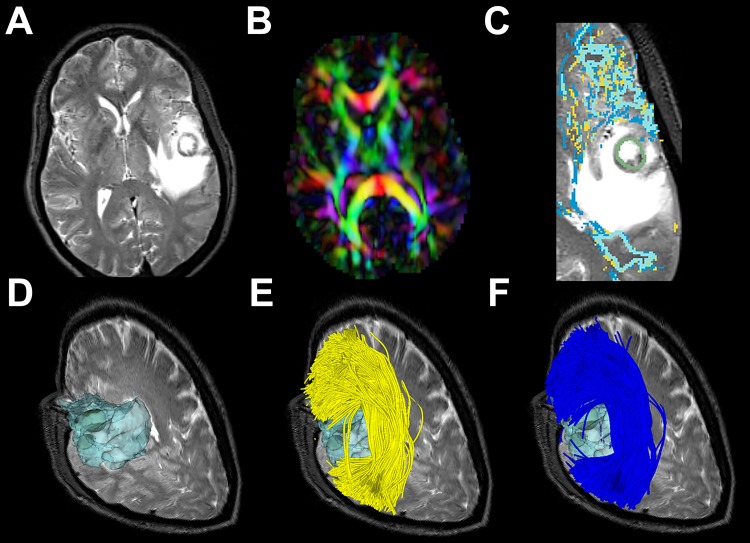
Purpose: Peritumoral edema impedes the full delineation of fiber tracts due to partial volume effects in image voxels that contain a mixture of cerebral parenchyma and extracellular water. The purpose of this study is to investigate the effect of incorporating a free water (FW) model of edema for white matter tractography in the presence of edema.
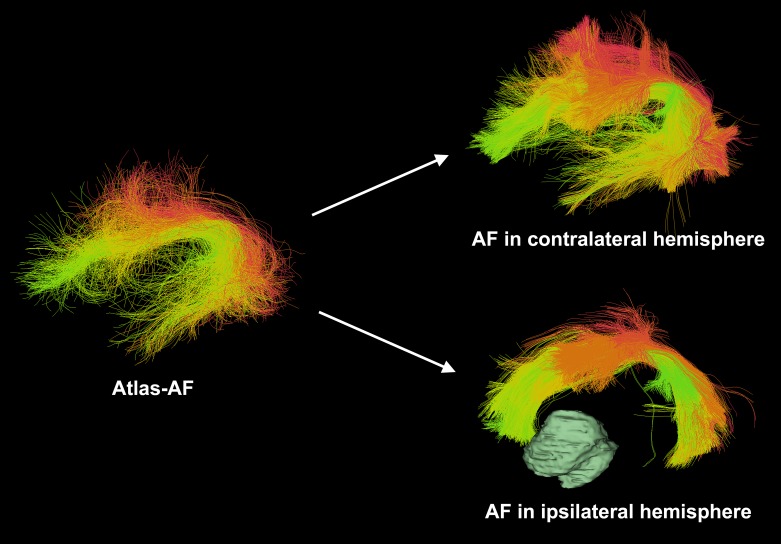
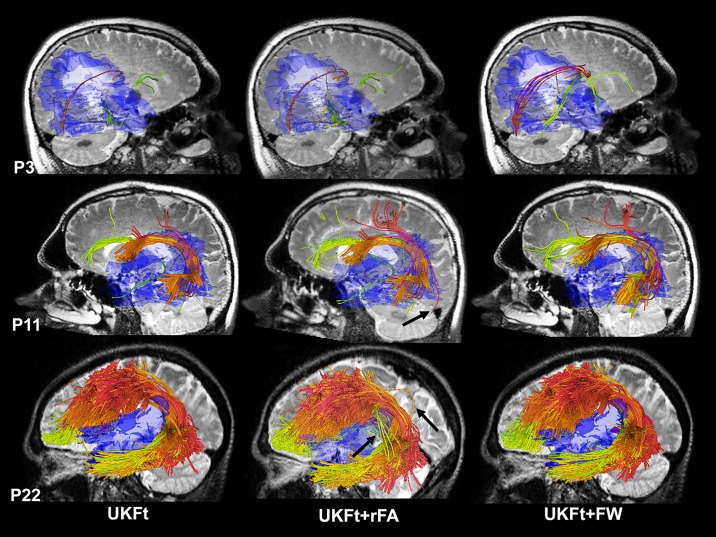
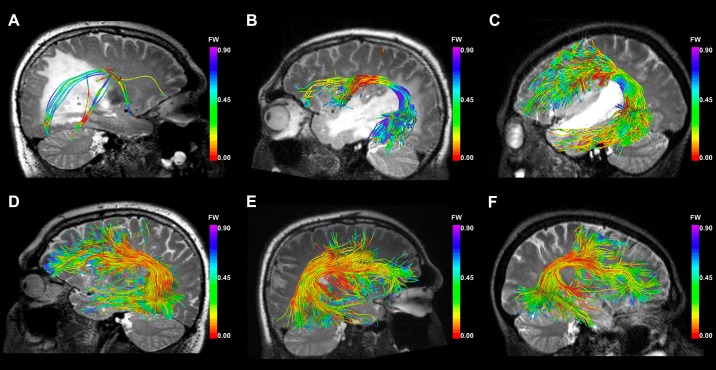
Materials and methods: We retrospectively evaluated 26 consecutive brain tumor patients with diffusion MRI and T2-weighted images acquired presurgically. Tractography of the arcuate fasciculus (AF) was performed using the two-tensor unscented Kalman filter tractography (UKFt) method, the UKFt method with a reduced fiber tracking stopping fractional anisotropy (FA) threshold (UKFt+rFA), and the UKFt method with the addition of a FW compartment (UKFt+FW). An automated white matter fiber tract identification approach was applied to delineate the AF. Quantitative measurements included tract volume, edema volume, and mean FW fraction. Visual comparisons were performed by three experts to evaluate the quality of the detected AF tracts.
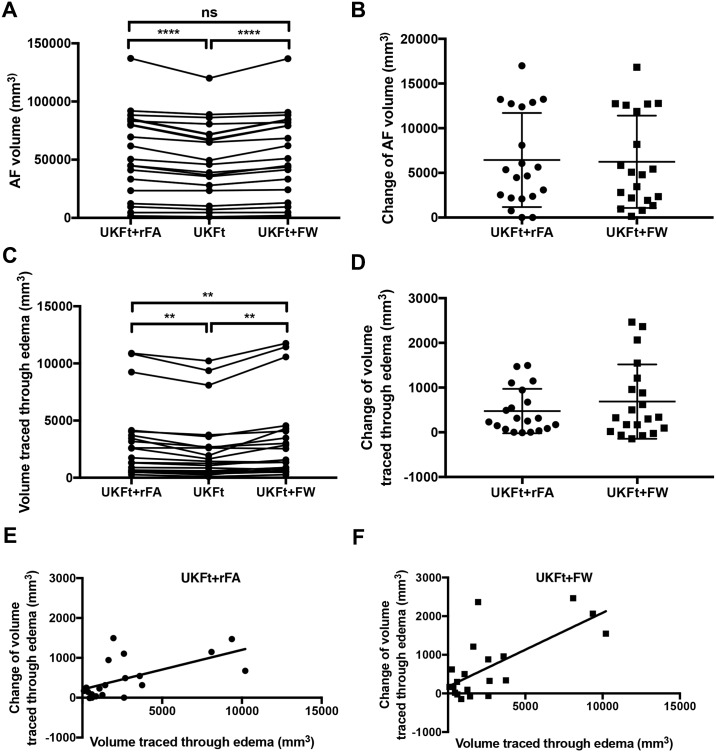
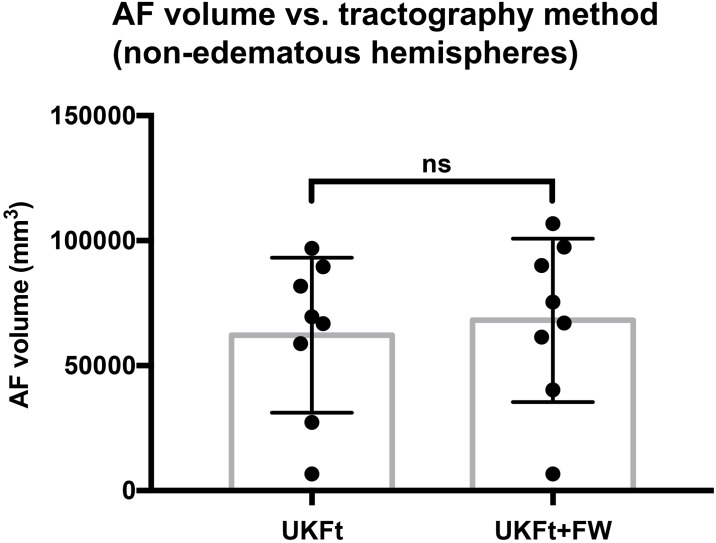
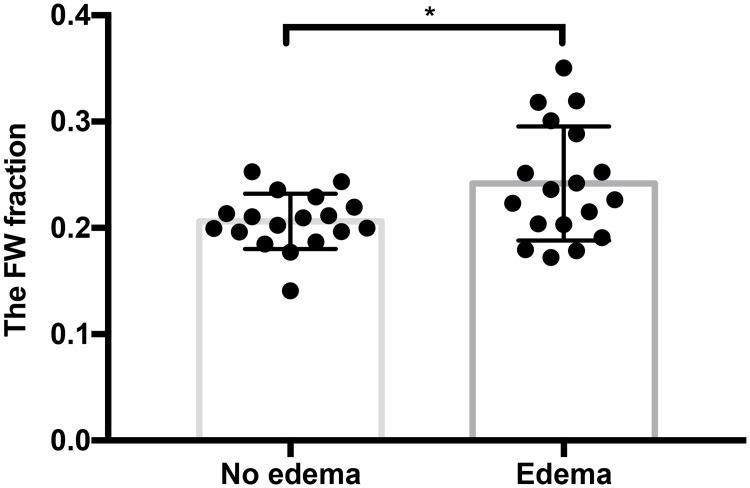
Results: The AF volume in edematous brain hemispheres was significantly larger using the UKFt+FW method (p<0.0001) compared to UKFt, but not significantly larger (p = 0.0996) in hemispheres without edema. The AF size increase depended on the volume of edema: a significant correlation was found between AF volume affected by (intersecting) edema and AF volume change with the FW model (Pearson r = 0.806, p<0.0001). The mean FW fraction was significantly larger in tracts intersecting edema (p = 0.0271). Compared to the UKFt+rFA method, there was a significant increase of the volume of the AF tract that intersected the edema using the UKFt+FW method, while the whole AF volumes were similar. Expert judgment results, based on the five patients with the smallest AF volumes, indicated that the expert readers generally preferred the AF tract obtained by using the FW model, according to their anatomical knowledge and considering the potential influence of the final results on the surgical route.
Conclusion: Our results indicate that incorporating biophysical models of edema can increase the sensitivity of tractography in regions of peritumoral edema, allowing better tract visualization in patients with high grade gliomas and metastases.
Conflict of interest statement
Figures
References
-
- Matthews PM, Honey GD, Bullmore ET. Applications of fMRI in translational medicine and clinical practice. Nat Rev Neurosci. 2006;7: 732–744. doi: 10.1038/nrn1929 - DOI - PubMed
-
- Farshidfar Z, Faeghi F, Mohseni M, Seddighi A, Kharrazi HH, Abdolmohammadi J. Diffusion tensor tractography in the presurgical assessment of cerebral gliomas. Neuroradiol J. 2014;27: 75–84. doi: 10.15274/NRJ-2014-10008 - DOI - PMC - PubMed
-
- Niu C, Liu X, Yang Y, Zhang K, Min Z, Wang M, et al. Assessing Region of Interest Schemes for the Corticospinal Tract in Patients With Brain Tumors. Medicine. 2016;95: e3189 doi: 10.1097/MD.0000000000003189 - DOI - PMC - PubMed
-
- Petrella JR, Shah LM, Harris KM, Friedman AH, George TM, Sampson JH, et al. Preoperative functional MR imaging localization of language and motor areas: effect on therapeutic decision making in patients with potentially resectable brain tumors. Radiology. 2006;240: 793–802. doi: 10.1148/radiol.2403051153 - DOI - PubMed
-
- Wu J-S, Zhou L-F, Tang W-J, Mao Y, Hu J, Song Y-Y, et al. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: a prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery. 2007;61: 935–48; discussion 948–9. doi: 10.1227/01.neu.0000303189.80049.ab - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- R21 CA198740 /NH/NIH HHS/United States
- R03 NS088301/NS/NINDS NIH HHS/United States
- U01 NS083223 /NH/NIH HHS/United States
- P41 EB015898 /NH/NIH HHS/United States
- P41 EB015898/EB/NIBIB NIH HHS/United States
- R03 NS088301 /NH/NIH HHS/United States
- U01 CA199459 /NH/NIH HHS/United States
- R01 MH097979/MH/NIMH NIH HHS/United States
- R25 CA089017 /NH/NIH HHS/United States
- R01 MH108574 /NH/NIH HHS/United States
- R25 CA089017/CA/NCI NIH HHS/United States
- P41 EB015902 /NH/NIH HHS/United States
- R01 MH074794/MH/NIMH NIH HHS/United States
- R01 MH074794 /NH/NIH HHS/United States
- U01 NS083223/NS/NINDS NIH HHS/United States
- R01 MH097979 /NH/NIH HHS/United States
- R01 MH108574/MH/NIMH NIH HHS/United States
- U01 CA199459/CA/NCI NIH HHS/United States
- P41 EB015902/EB/NIBIB NIH HHS/United States
- R21 CA198740/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
