

Classical fragile-X phenotype in a female infant disclosed by comprehensive genomic studies
- PMID: 29747568
- PMCID: PMC5946481
- DOI: 10.1186/s12881-018-0589-6
Classical fragile-X phenotype in a female infant disclosed by comprehensive genomic studies
Abstract
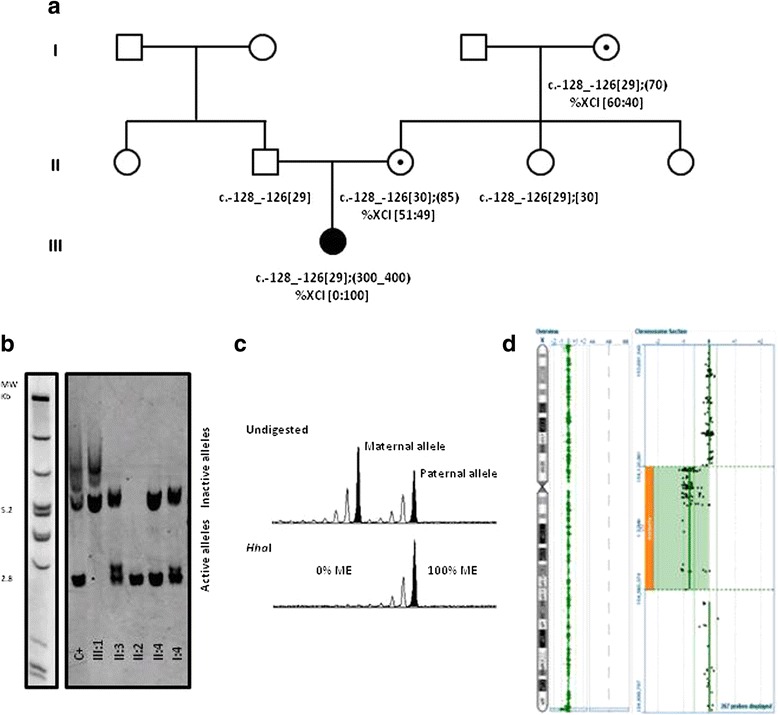
Background: We describe a female infant with Fragile-X syndrome, with a fully expanded FMR1 allele and preferential inactivation of the homologous X-chromosome carrying a de novo deletion. This unusual and rare case demonstrates the importance of a detailed genomic approach, the absence of which could be misguiding, and calls for reflection on the current clinical and diagnostic workup for developmental disabilities.
Case presentation: We present a female infant, referred for genetic testing due to psychomotor developmental delay without specific dysmorphic features or relevant family history. FMR1 mutation screening revealed a methylated full mutation and a normal but inactive FMR1 allele, which led to further investigation. Complete skewing of X-chromosome inactivation towards the paternally-inherited normal-sized FMR1 allele was found. No pathogenic variants were identified in the XIST promoter. Microarray analysis revealed a 439 kb deletion at Xq28, in a region known to be associated with extreme skewing of X-chromosome inactivation.
Conclusions: Overall results enable us to conclude that the developmental delay is the cumulative result of a methylated FMR1 full mutation on the active X-chromosome and the inactivation of the other homologue carrying the de novo 439 kb deletion. Our findings should be taken into consideration in future guidelines for the diagnostic workup on the diagnosis of intellectual disabilities, particularly in female infant cases.
Keywords: Developmental disabilities in females; FMR1 methylated full mutation; Fragile-X syndrome; Skewing of X-chromosome inactivation; Xq28 deletion.
Conflict of interest statement
Ethics approval and consent to participate
Proband’s parents, signed informed consent for the use of DNA samples in intellectual disability research. This study has been approved by the medical ethical committee of the Centro Hospitalar do Porto (CHP, E.P.E.) - REF 2014.203 (144-DEFI/173-CES).
Consent for publication
Proband’s parents, signed informed consent for publication that includes medical information and photographs.
Competing interests
Dr. Paula Jorge is an Associate Editor for BMC Medical Genetics. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- AJMH V, Pieretti M, Sutcliffe JS, Fu Y-H, DPA K, Pizzuti A, Reiner O, Richards S, Victoria MF, Zhang F, Eussen BE, G-JB v O, LAJ B, Riggins GJ, Chastain JL, Kunst CB, Galjaard H, Thomas Caskey C, Nelson DL, Oostra BA, Warren ST. Identification of a gene (FMR-1) containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile X syndrome. Cell. 1991;65(5):905–914. doi: 10.1016/0092-8674(91)90397-H. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
