

High prevalence of cesarean section births in private sector health facilities- analysis of district level household survey-4 (DLHS-4) of India
- PMID: 29747609
- PMCID: PMC5946478
- DOI: 10.1186/s12889-018-5533-3
High prevalence of cesarean section births in private sector health facilities- analysis of district level household survey-4 (DLHS-4) of India
Abstract
Background: Worldwide rising cesarean section (CS) births is an issue of concern. In India, with increase in institutional deliveries there has also been an increase in cesarean section births. Aim of the study is to quantify the prevalence of cesarean section births in public and private health facility, and also to determine the factors associated with cesarean section births.
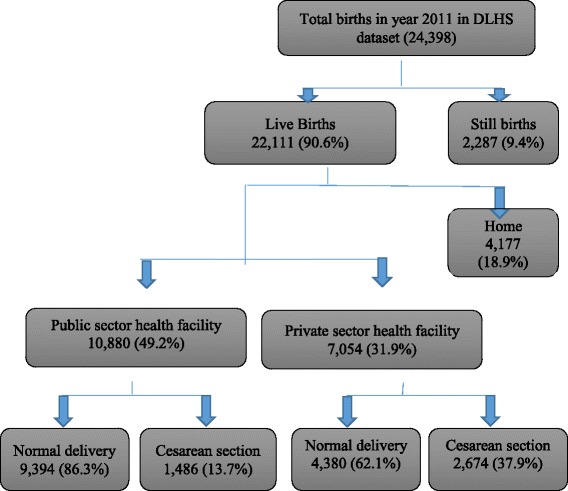
Methods: We analyzed data from district level household survey data 4 (DLHS-4) combined individual level dataset for 19 states/UTs of India comprising 24,398 deliveries resulting in 22,111 live births for year 2011. The percentages and Chi-square has been computed for the select variables viz. Socio demographic, maternal, antenatal care and delivery related based on type of births (CS Vs normal births). The multiple logistic regression model has been used to identify the potential risk factors associated with CS births.
Results: Of 22,111 live birth analyzed 49.2% were delivered at public sector, 31.9% at private sector and 18.9% were home deliveries. Prevalence of CS births were 13.7% (95% CI; 13.0- 14.3%) and 37.9% (95% CI; 36.7- 39.0%) in the public and private sectors, respectively. Higher odds of CS births were observed with- delivery at private health facility (OR 3.79; 95% C.I 3.06-4.72), urban residence (OR 1.15; 95% C.I 1.00- 1.35), first delivery after 35 years of maternal age (OR 5.5; 95% C.I 1.85- 16.4), hypertension in pregnancy (OR 1.32; 95% C.I 1.06- 1.65) and breach presentation (OR 2.37; 95% C.I. 1.63- 3.43).
Conclusions: Our findings shows that CS births are nearly three times more in private as compared to public sector health facilities.The higher rates of CS births, especially in private sector, not only increase the cost of care but may pose unnecessary risks to women (when there is no indications for CS). The government of India need to take measures to strengthen existing public health facilities as well as ensure that cesarean sections are performed based upon medical indications in both public and private sector health facilities.
Keywords: Cesarean section; Normal delivery; Prevalence; Private sector; Public sector.
Conflict of interest statement
Ethics approval and consent to participate
The DLHS-4 was collected by the International Institute for Population Sciences, Mumbai on behalf of the Ministry of Health and Family Welfare, Government of India. All data were de-identified. The de-identified version of the DLHS-4 data is publicly available upon formal request for access to the Director of India’s Institute of Population Sciences. As no patient could be identified or contacted, no ethics approval was required by individual researchers to undertake this study (Please refer page no- 36 of the document National ethical guidelines for biomedical and health research involving human participants link to the document-
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Souza J, Gulmezoglu A, Lumbiganon P, et al. Cesarean section without medical indications is associated with an increased risk of adverse short-term maternal outcomes: the 2004-2008 WHO global survey on maternal and perinatal health. BMC Med. 2010;8:71. doi: 10.1186/1741-7015-8-71. - DOI - PMC - PubMed
-
- World Health Organization. WHO Statement on Cesarean Section Rates, 2015, Available from: http://apps.who.int/iris/bitstream/10665/161442/1/WHO_RHR_15.02_eng.pdf. [Last Accessed 17 Aug 2017].
-
- World Health Organization Appropriate technology for birth. Lancet. 1985;2:436–7. - PubMed
-
- Neuman M, Alcock G, Azad K, Kuddus A, Osrin D, More NS, Nair N, Tripathy P, Sikorski C, Saville N, Sen A. Prevalence and determinants of cesarean section in private and public health facilities in underserved south Asian communities: cross-sectional analysis of data from Bangladesh, India and Nepal. BMJ Open. 2014;4(12):e005982. doi: 10.1136/bmjopen-2014-005982. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
