

Haemodynamically Derived Pulmonary Artery Pulsatility Index Predicts Mortality in Pulmonary Arterial Hypertension
- PMID: 29748060
- PMCID: PMC7175917
- DOI: 10.1016/j.hlc.2018.04.280
Haemodynamically Derived Pulmonary Artery Pulsatility Index Predicts Mortality in Pulmonary Arterial Hypertension
Abstract
Background: Pulmonary artery (PA) pulsitility index (PAPi) is a novel haemodynamic index shown to predict right ventricular failure in acute inferior myocardial infarction and post left ventricular assist device surgery. We hypothesised that PAPi calculated as [PA systolic pressure - PA diastolic pressure]/right atrial pressure (RAP) would be associated with mortality in the National Institutes of Health Registry for Primary Pulmonary Hypertension (NIH-RPPH).
Methods: The impact of PAPi, the Pulmonary Hypertension Connection (PHC) risk score, right ventricular stroke work, pulmonary artery capacitance (PAC), other haemodynamic indices, and demographic characteristics was evaluated in 272 NIH-RPPH patients using multivariable Cox proportional hazards (CPH) regression and receiver operating characteristic (ROC) analysis.
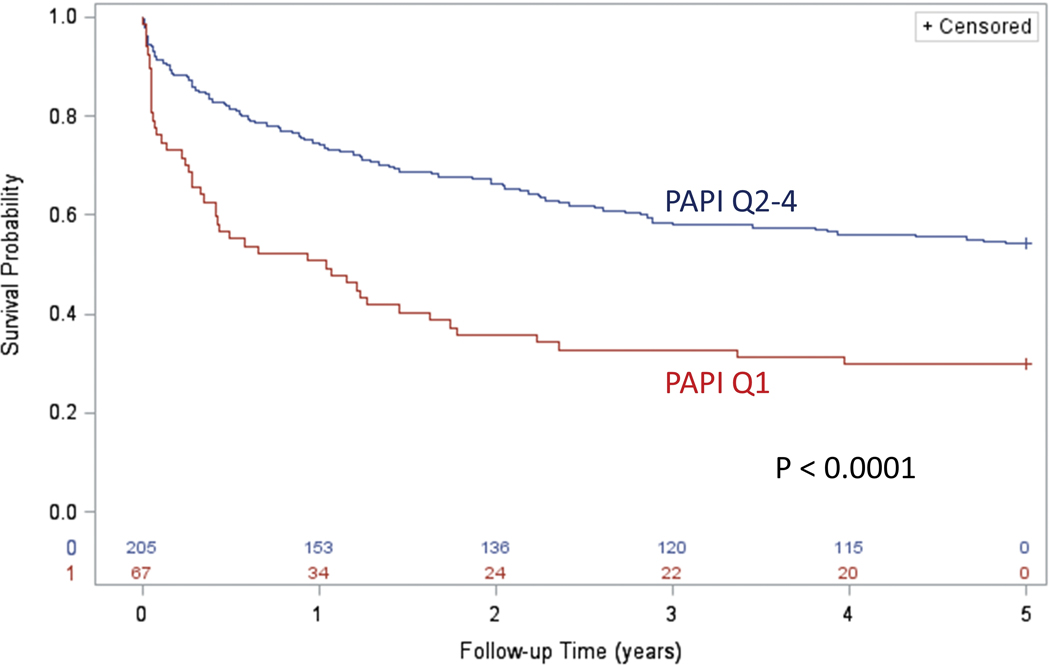
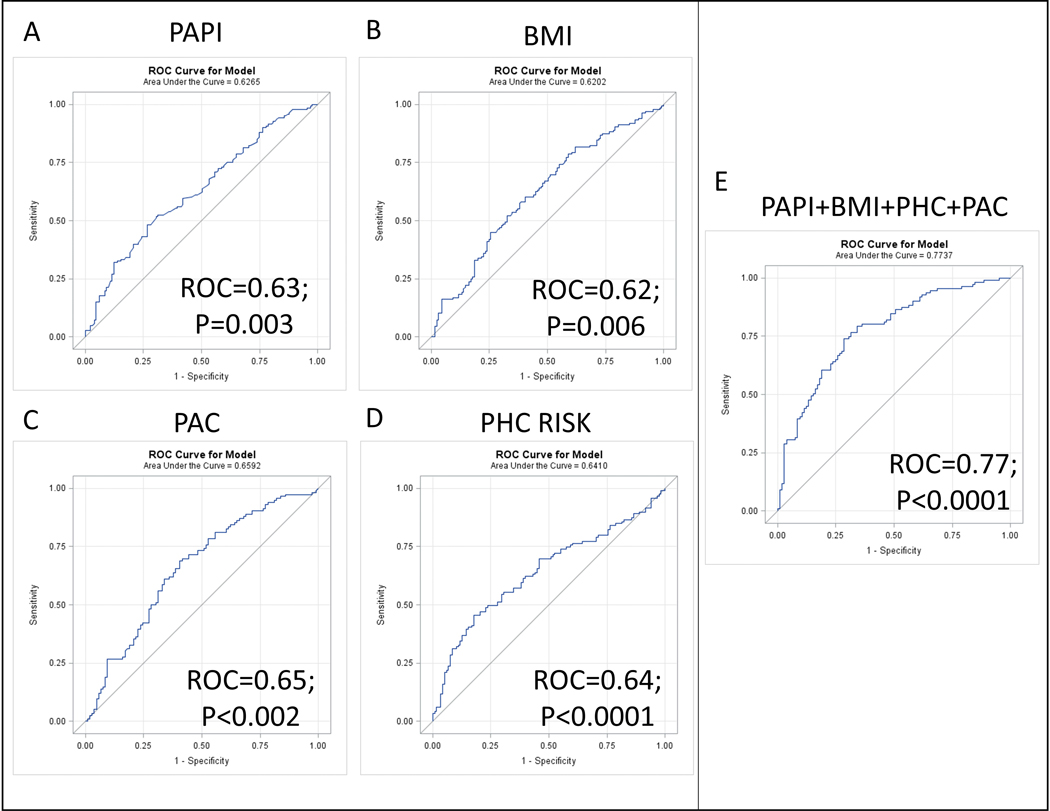
Results: In the 272 patients (median age 37.7+/-15.9years, 63% female), the median PAPi was 5.8 (IQR 3.7-9.2). During 5years of follow-up, 51.8% of the patients died. Survival was markedly lower (32.8% during the first 3years) in PAPi quartile 1 compared with the remaining patients (58.5% over 3years in quartiles 2-4; p<0.0001). The best multivariable CPH survival model included PAPi, the PHC-Risk score, PAC, and body mass index (BMI). In this model, the adjusted hazard ratio for death with increasing PAPi was 0.946 (95% CI 0.905-0.989). The independent ROC areas for 5-year survival based on bivariable logistic regression for PAPi, BMI, PHC Risk, and PAC were 0.63, 0.62, 0.64, and 0.65, respectively (p<0.01). The ROC area for 5-year survival for the multivariable logistic model with all four covariates was 0.77 (p<0.0001).
Conclusions: Pulmonary artery pulsatility index was independently associated with survival in PAH, highlighting the utility of PAPi in combination with other key measures for risk stratification in this population.
Keywords: Heart failure; PAPi; Pulmonary hypertension.
Copyright © 2018 Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) and the Cardiac Society of Australia and New Zealand (CSANZ). Published by Elsevier B.V. All rights reserved.
Figures


References
-
- Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436–1448. - PubMed
-
- Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J Med. 2004;351(16):1655–1665. - PubMed
-
- D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115(5):343–349. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 2010;122(2):164–172. - PubMed
-
- Sachdev A, Villarraga HR, Frantz RP, et al. Right ventricular strain for prediction of survival in patients with pulmonary arterial hypertension. Chest. 2011;139(6):1299–1309. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
